
Page 1127 - TNFlipTest
P. 1127
Toronto Notes 2019
Skin Lesions and Masses
Plastic Surgery PL5
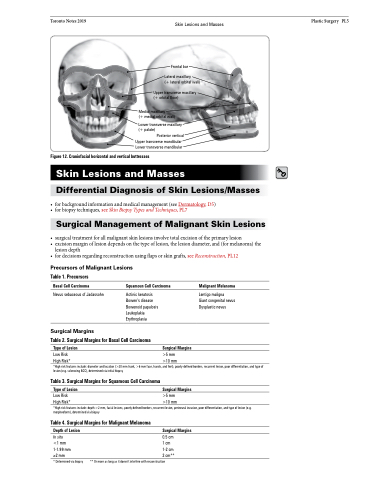
Frontal bar
Lateral maxillary
(+ lateral orbital wall)
Upper transverse maxillary (+ orbital floor)
Medial maxillary
(+ medial orbital wall)
Lower transverse maxillary (+ palate)
Posterior vertical Upper transverse mandibular Lower transverse mandibular
Figure 12. Craniofacial horizontal and vertical buttresses
Skin Lesions and Masses
Differential Diagnosis of Skin Lesions/Masses
• forbackgroundinformationandmedicalmanagement(seeDermatology,D5)
• forbiopsytechniques,seeSkinBiopsyTypesandTechniques,PL7
Surgical Management of Malignant Skin Lesions
• surgicaltreatmentforallmalignantskinlesionsinvolvetotalexcisionoftheprimarylesion
• excisionmarginoflesiondependsonthetypeoflesion,thelesiondiameter,and(formelanoma)the
lesion depth
• fordecisionsregardingreconstructionusingflapsorskingrafts,seeReconstruction,PL12
Precursors of Malignant Lesions
Table 1. Precursors
Basal Cell Carcinoma
Nevus sebaceous of Jadassohn
Surgical Margins
Squamous Cell Carcinoma
Malignant Melanoma
Lentigo maligna
Giant congenital nevus Dysplastic nevus
Actinic keratosis Bowen’s disease Bowenoid papulosis Leukoplakia Erythroplasia
Table 2. Surgical Margins for Basal Cell Carcinoma
Type of Lesion
Surgical Margins
Low Risk
High Risk*
*High risk features include: diameter and location (>20 mm trunk, >6 mm face, hands, and feet), poorly defined borders, recurrent lesion, poor differentiation, and type of lesion (e.g. sclerosing BCC), determined via initial biopsy
Table 3. Surgical Margins for Squamous Cell Carcinoma
Type of Lesion
Low Risk
High Risk*
*High risk features include: depth >2 mm, facial lesions, poorly defined borders, recurrent lesion, perineural invasion, poor differentiation, and type of lesion (e.g. morpheoform), determined via biopsy
>5 mm >10 mm
Table 4. Surgical Margins for Malignant Melanoma
Surgical Margins
>5 mm >10 mm
Depth of Lesion
In situ
<1 mm 1-1.99 mm
≥2 mm
* Determined via biopsy
Surgical Margins
0.5 cm 1 cm 1-2 cm
2 cm** ** Or more as long as it doesn’t interfere with reconstruction
© Julian Kirk-Elleker 2006
