
Page 292 - TNFlipTest
P. 292
E50 Endocrinology Common Medications Toronto Notes 2019 Common Medications
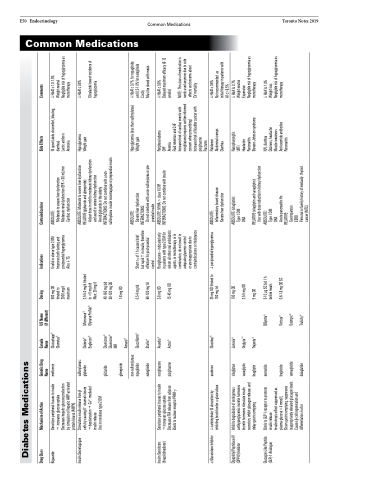
Diabetes Medications
Drug Class
Mechanism of Action
Generic Drug Name metformin
Canada Name Glucophage® Glumetza®
US Name (if different)
Dosing
Indications
Contraindications
Side Effects
Comments
Biguanide
Sensitizes peripheral tissues to insulin g increases glucose uptake Decreases hepatic glucose production by simulation of hepatic AMP-activated protein kinase (AMPK)
500 mg OD titrated to 2000 mg/d maximum
Useful in obese type 2 DM Improves both fasting and postprandial hyperglycemia AlsoTG
ABSOLUTE:
Moderate to severe liver dysfunction Moderate renal dysfunction GFR <30 mL/min Cardiac dysfunction
GI upset (abdo discomfort, bloating, diarrhea)
Lactic acidosis
Anorexia
HbA1c 1.0-1.5%
Weight neutral
Negligible risk of hypoglycemia as monotherapy
Insulin Secretagogue
Stimulates insulin release from β cells by causing K+ channel closure gdepolarizationgCa2+ mediated insulin release
sulfonylureas: glyburide
ABSOLUTE: Moderate to severe liver dysfunction RELATIVE (glyburide and glimepiride):
Hypoglycemia Weight gain
HbA1c 0.8%
Glicalazide lowest incidence of
Insulin Sensitizers (thiazolidinedione)
Sensitizes peripheral tissues to insulin gincreases glucose uptake Decreases FFA release from adipose Binds to nuclear receptor PPAR-γ
ABSOLUTE: NYHA > class II CHF INTERACTIONS: Do not combine with insulin
Peripheral edema
CHF
Anemia
Fluid retention and CHF
Increased risk of cardiac events with rosiglitazone (requires written informed consent when prescribing)
HbA1c 0.8%
Delayed maximum efficacy (6-12 weeks)
Use in nonobese type 2 DM
α-GlucosidaseInhibitor carbohydrateGIabsorptionby inhibiting brush border α-glucosidase
acarbose
Glucobay®
25mgODtitratedto postprandialhyperglycemia 100 mg tid
ABSOLUTE:
Inflammatory bowel disease Severe liver dysfunction
HbA1c 0.6%
Not recommended as
initial therapy in patients with A1c>8.5%
HbA1c 0.7%
Weight neutral
Expensive
Negligible risk of hypoglycemia as monotherapy
Dipeptidyl Peptidase-IV (DPP-IV) Inhibitor
Inhibits degradation of endogenous antihyperglycemic incretin hormones Incretin hormones stimulate insulin secretion, inhibit glucagon release, and delay gastric emtyping
sitagliptan saxagliptin linagliptin exenatide
Januvia® OnglyzaTM Trajenta®
100 mg OD
ABSOLUTE (sitagliptin): Type 1 DM
DKA
Nasopharyngitis
URTI
Headache
Pancreatitis
Stevens Johnson syndrome
Glucagon-Like Peptide (GLP)-1 Analogue
Binds to GLP-1 receptor to promote insulin release
Insulinotropic effect suppressed as plasma glucose <4 mmol/L
BByetta®
5-10 μg SC bid 1 h before meals
ABSOLUTE:
Type 1 DM
DKA
Acute pancreatitis Hx
N/V, diarrhea
Dizziness, headache Muscle weakness Anti-exentide antibodies Pancreatitis
HbA1c 1.0%
Weight loss
Negligible risk of hypoglycemia as monotherapy
Slows gastric emptying, suppresses inappropriately elevated glucagon levels Causes β-cell regeneration and differentiation in vitro
RELATIVE:
Gastroparesis
ESRD
Personalorfamilyhistoryofmedually thyroid cancer (MTC)
gliclazide
Diamicron® Diamicron® MR
40-160 mg bid 30-120 mg OD
INTERACTIONS: Do not combine with a non- sulfonylurea insulin secretagogue or preprandial insulin
glimepiride
1-8 mg OD
non-sulfonylureas: repaglinide
Amaryl® GlucoNorm® Starlix® Avandia® Actos®
0.5-4 mg tid 60-120 mg tid 2-8 mg OD 15-45 mg OD
Short t1/2 of 1 h causes brief but rapid in insulin, therefore effective for post-prandial control
Rosiglitazone – indicated only in patients with type 2 DM for whom all other oral antidiabetic agents, in monotherapy or in combination, do not result in adequate glycemic control
or are inappropriate due to contraindications or intolerance
ABSOLUTE:
Severe liver dysfunction
Hypoglycemia (less than sulfonylurea) Weight gain
HbA1c 0.7% for repaglinide and 0.5-1.0% for nateglinide Costly
Must be dosed with meals
nateglinide rosiglitazone pioglitazone
INTERACTIONS:
Do not combine with a non-sulfonylurea or pre- prandial insulin
liraglutide semaglutide dulaglutide
Victoza® Ozempic® Trulicity®
0.6-1.8 mg OD SC
Diabeta® Euglucon®
Micronase® Glynase PreTab®
2.5-5.0 mg/d titrated to >5 mg bid
Max: 20 mg/d
Adjust dose in mild to moderate kidney dysfunction and avoid in severe kidney dysfunction
Avoid glyburide in the elderly
2.5-5 mg OD
5 mg OD
RELATIVE (sitagliptin and saxagliptin):
Use with dose reduction in kidney dysfunction
Increased risk of bladder cancer with pioglitazone
Fractures
Flatulence
effects and oncerns about CV mortality
Abdominal cramps Diarrhea
hypoglycemia
NOTE: This class of medication is rarely used anymore due to side
