
Page 387 - TNFlipTest
P. 387
Toronto Notes 2019 Liver
Complications
• hematologicchangesincirrhosis
■ pancytopenia from hypersplenism: platelets first, then WBC, then hemoglobin
■ decreased clotting factors resulting in elevated INR
■ relationship of INR to bleeding tendency is controversial; some patients may be hypocoagulable,
others may be hypercoagulable • varicealbleeds
■ half of patients with cirrhosis have gastroesophageal varices and one-third of these develop hemorrhage with an overall mortality of >30%
■ hepatic venous pressure gradient (HVPG) ≥10 mmHg is the strongest predictor of variceal development
■ treatment: resuscitation, antibiotic prophylaxis, vasoactive drugs (e.g. octreotide IV) combined with endoscopic band ligation or sclerotherapy, Transjugular Intrahepatic Portosystemic Shunt (TIPS)
• renalfailureincirrhosis ■ classifications
pre-renal (usually due to over-diuresis) ◆ acute tubular necrosis
◆ Hepatorenal Syndrome (HRS)
– Type I: sudden and acute renal failure (rapid doubling of creatinine over 2 wk)
– Type II: gradual increase in creatinine with worsening liver function (creatinine doubling
over years)
◆ HRS can occur at any time in severe liver disease, especially after:
– overdiuresis or dehydration, such as diarrhea, vomiting, etc. – GI bleed
– sepsis
◆ treatment for hepatorenal syndrome (generally unsuccessful at improving long-term survival) – for type I HRS: octreotide + midodrine + albumin (increases renal blood flow by increasing
systemic vascular resistance)
– definitive treatment is liver transplant
• hepatopulmonarysyndrome
■ majority of cases due to cirrhosis, though can be due to other chronic liver diseases, such as non-
cirrhotic portal HTN
■ thought to arise from ventilation-perfusion mismatch, intrapulmonary shunting and limitation of
oxygen diffusion, failure of damaged liver to clear circulating pulmonary vasodilators vs. production
of a vasodilating substance by the liver
■ clinical features
◆ hyperdynamic circulation with cardiac output >7 L/min at rest and decreased pulmonary + systemic resistance (intrapulmonary shunting)
◆ dyspnea, platypnea (increase in dyspnea in upright position, improved by recumbency), and orthodeoxia (desaturation in the upright position, improved by recumbency)
◆ diagnosis via contrast-enhanced echocardiography: inject air bubbles into peripheral vein; air bubbles appear in left ventricle after third heartbeat (normal = no air bubbles; in ventricular septal defect, air bubbles seen <3 heart beats)
Gastroenterology G37
Usual causes of death in cirrhosis: renal failure (hepatorenal syndrome), sepsis, GI bleed, or HCC
Hepatorenal Syndrome vs. Pre-Renal Failure – Difficult to Differentiate
• Similar blood and urine findings
• Urine sodium: very low in hepatorenal; low
in pre-renal
• Intravenous fluid challenge: giving volume
expanders improves pre-renal failure, but not hepatorenal syndrome
Hepatopulmonary Syndrome
Clinical Triad
• Liver disease
• Increased alveolar-arterial gradient while
breathing room air
• Evidence for intrapulmonary vascular
abnormalities
Fibrosis may regress and disappear if cause of liver injury is treated or resolves
◆ only proven treatment is liver transplantation
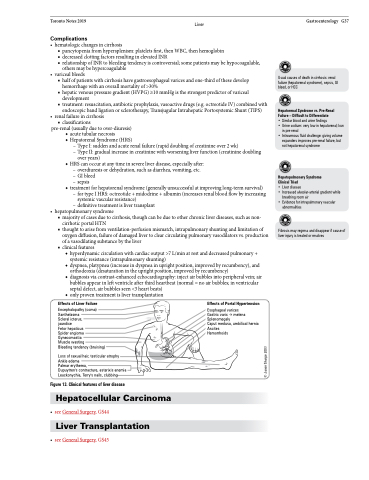
Effects of Liver Failure
Encephalopathy (coma) Xanthelasma
Scleral icterus, jaundice
Fetor hepaticus
Spider angioma Gynecomastia
Muscle wasting
Bleeding tendency (bruising)
Loss of sexual hair, testicular atrophy Ankle edema
Palmar erythema,
Dupuytren's contracture, asterixis anemia Leuckonychia, Terry's nails, clubbing
Figure 13. Clinical features of liver disease
Hepatocellular Carcinoma
• seeGeneralSurgery,GS44
Liver Transplantation
Effects of Portal Hypertension
Esophageal varices
Gastric varix melena Splenomegaly
Caput medusa, umbilical hernia Ascites
Hemorrhoids
• seeGeneralSurgery,GS45
© Jason Sharpe 2003
