
Page 498 - TNFlipTest
P. 498
GY12 Gynecology
Endometriosis
Toronto Notes 2019
Endometriosis – Take Home Points
• Suggestive history even with a negative exam should be considered adequate for a presumptive diagnosis
• Pelvic pain that is not primary dysmenorrhea should be considered endometriosis until proven otherwise
• Medical management is the mainstay of endometriosis
Sites of Occurrence
• ovaries:60%patientshaveovarianinvolvement
• broadligament,vesicoperitonealfold
• peritonealsurfaceofthecul-de-sac,uterosacralligaments
• rectosigmoidcolon,appendix
• rarelymayoccurinsitesoutsideabdomen/pelvis,includinglungs
Clinical Features
• maybeasymptomaticandcanoccurwithoneof3presentations
1. pain
■ menstrual symptoms
◆ cyclic symptoms due to growth and bleeding of ectopic endometrium, usually precede menses
(24-48 h) and continue throughout and after flow
◆ secondary dysmenorrhea
◆ sacral backache with menses
◆ pain may eventually become chronic, worsening perimenstrually ◆ deep dyspareunia
■ bowel and bladder symptoms
◆ frequency, dysuria, hematuria
◆ cyclic diarrhea/constipation, hematochezia, dyschezia (suggestive of deeply infiltrating disease)
2. infertility
■ 30-40% of patients with endometriosis will be infertile
■ 15-30% of those who are infertile will have endometriosis
3. mass (endometrioma)
■ ovarian mass can present with any of above symptoms or be asymptomatic
■ physical
■ tender nodularity of uterine ligaments and cul-de-sac felt on rectovaginal exam
■ fixed retroversion of uterus
■ firm, fixed adnexal mass (endometrioma: an endometriotic cyst encompassing ovary)
Investigations
• definitivediagnosiscanbemadebasedon:
■ direct visualization of lesions typical of endometriosis at laparoscopy
■ biopsy and histologic exam of specimens (2 or more of: endometrial epithelium, glands, stroma,
hemosiderin-laden macrophages) • laparoscopy
■ mulberry spots: dark blue or brownish-black implants on the uterosacral ligaments, cul-de-sac, or anywhere in the pelvis
■ endometrioma: “chocolate” cysts on the ovaries ■ “powder-burn” lesions on the peritoneal surface ■ early white lesions and clear blebs
■ peritoneal “pockets”
• CA-125
■ may be elevated in patients with endometriosis but should NOT be used as a diagnostic test
Laparoscopy for diagnosis and treatment
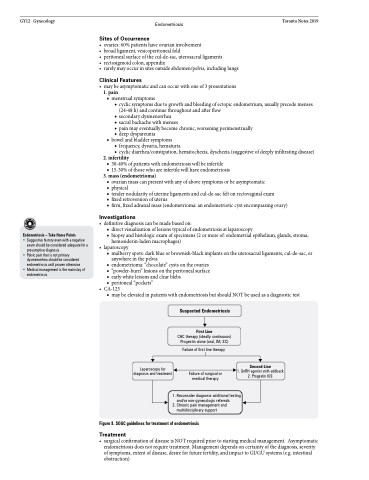
Suspected Endometriosis
First Line
CHC therapy (ideally continuous) Progestin alone (oral, IM, SC)
Failure of first line therapy
Failure of surgical or medical therapy
Second Line
1. GnRH agonist with addback 2. Progestin IUS
1. Reconsider diagnosis additional testing and/or non-gynecologic referrals
2. Chronic pain management and multidisciplinary support
Figure 8. SOGC guidelines for treatment of endometriosis
Treatment
• surgical confirmation of disease is NOT required prior to starting medical management. Asymptomatic endometriosis does not require treatment. Management depends on certainty of the diagnosis, severity of symptoms, extent of disease, desire for future fertility, and impact to GI/GU systems (e.g. intestinal obstruction)
