
Page 960 - TNFlipTest
P. 960
OR26 Orthopedics
Spine Toronto Notes 2019
LUMBAR DISC HERNIATION
• tearinannulusfibrosusallowsprotrusionofnucleuspulposus,causingeitheracentral,posterolateral, or lateral disc herniation, most commonly at L5-S1 > L4-5 > L3-4
• 3:1 male to female
• only5%becomesymptomatic
• usuallyahistoryofflexion-typeinjury
Clinical Features
• backdominantpain(centralherniation)orlegdominantpain(lateralherniation) • tendernessbetweenspinousprocessesataffectedlevel
• musclespasm±lossofnormallumbarlordosis
• neurologicaldisturbanceissegmentalandvarieswithlevelofcentralherniation
■ motor weakness (L4, L5, S1)
■ diminished reflexes (L4, S1)
■ diminished sensation (L4, L5, S1)
• positivestraightlegraise
• positivecontralateralSLR
• positiveLasegueandBowstringsign
• caudaequinasyndrome(presentin1-10%):surgicalemergency
Investigations
• X-ray,MRI,considerapost-voidresidualvolumetocheckforurinaryretention;post-void>100mL should heighten suspicion for cauda equina syndrome
Treatment
• non-operative
■ symptomatic
◆ extension protocol
◆ NSAIDS • operative
■ indication: progressive neurological deficit, failure of symptoms to resolve within 3 mo, or cauda equina syndrome due to central disc herniation
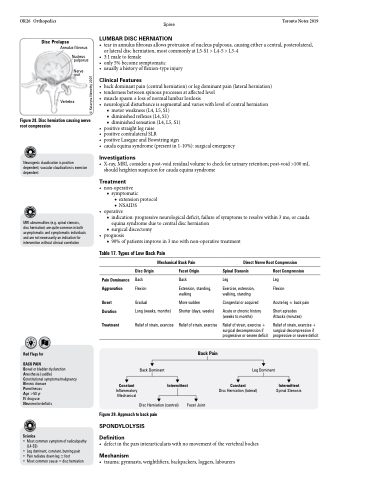
Disc Prolapse
Annulus fibrosus
Nucleus pulposus
Nerve root
Vertebra
Figure 28. Disc herniation causing nerve root compression
Neurogenic claudication is position dependent; vascular claudication is exercise dependent
MRI abnormalities (e.g. spinal stenosis, disc herniation) are quite common in both asymptomatic and symptomatic individuals and are not necessarily an indication for intervention without clinical correlation
■ surgical discectomy • prognosis
■ 90% of patients improve in 3 mo with non-operative treatment
Table 17. Types of Low Back Pain
Mechanical Back Pain
Direct Nerve Root Compression
Disc Origin
Back Flexion
Gradual
Long (weeks, months)
Relief of strain, exercise
Back Dominant
Facet Origin
Back
Extension, standing, walking
More sudden
Shorter (days, weeks)
Relief of strain, exercise
Spinal Stenosis
Leg
Exercise, extension, walking, standing
Congenital or acquired
Acute or chronic history (weeks to months)
Relief of strain, exercise + surgical decompression if progressive or severe deficit
Root Compression
Leg Flexion
Acute leg ± back pain
Short episodes Attacks (minutes)
Relief of strain, exercise + surgical decompression if progressive or severe deficit
Red Flags for
BACK PAIN
Bowel or bladder dysfunction Anesthesia (saddle)
Constitutional symptoms/malignancy Khronic disease
Paresthesias
Age >50 yr
IV drug use
Neuromotor deficits
Sciatica
• Most common symptom of radiculopathy (L4-S3)
• Leg dominant, constant, burning pain
• Pain radiates down leg ± foot
• Most common cause = disc herniation
Pain Dominance Aggravation
Onset Duration
Treatment
Constant
Inflammatory Mechanical
Back Pain
Leg Dominant
Intermittent
Constant
Intermittent
Spinal Stenosis
Disc Herniation (lateral)
Figure 29. Approach to back pain
SPONDYLOLYSIS Definition
Disc Herniation (central)
Facet Joint
• defectintheparsinterarticulariswithnomovementofthevertebralbodies
Mechanism
• trauma: gymnasts, weightlifters, backpackers, loggers, labourers
© Kataryna Nemethy 2007
