
Page 999 - TNFlipTest
P. 999
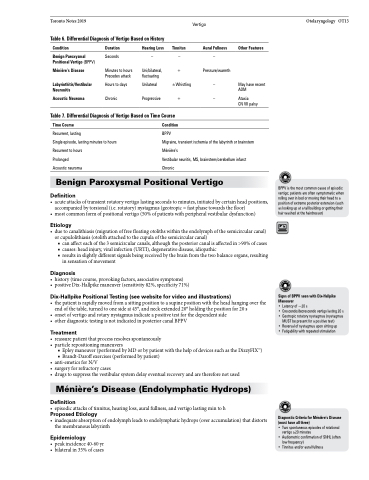
Toronto Notes 2019 Vertigo Table 6. Differential Diagnosis of Vertigo Based on History
Otolaryngology OT13
Condition
Benign Paroxysmal Positional Vertigo (BPPV)
Ménière’s Disease
Labyrinthitis/Vestibular Neuronitis
Acoustic Neuroma
Duration
Seconds
Minutes to hours Precedes attack
Hours to days Chronic
Hearing Loss Tinnitus Aural Fullness Other Features
–––
Uni/bilateral, + Pressure/warmth fluctuating
Unilateral ±Whistling – May have recent AOM
Progressive + – Ataxia
CN VII palsy
Table 7. Differential Diagnosis of Vertigo Based on Time Course
Time Course
Recurrent, lasting
Single episode, lasting minutes to hours Recurrent to hours
Prolonged
Acoustic neuroma
Condition
BPPV
Migraine, transient ischemia of the labyrinth or brainstem Ménière’s
Vestibular neuritis, MS, brainstem/cerebellum infarct Chronic
Benign Paroxysmal Positional Vertigo
Definition
• acuteattacksoftransientrotatoryvertigolastingsecondstominutes,initiatedbycertainheadpositions, accompanied by torsional (i.e. rotatory) nystagmus (geotropic = fast phase towards the floor)
• mostcommonformofpositionalvertigo(50%ofpatientswithperipheralvestibulardysfunction)
Etiology
• duetocanalithiasis(migrationoffreefloatingotolithswithintheendolymphofthesemicircularcanal) or cupulolithiasis (otolith attached to the cupula of the semicircular canal)
■ can affect each of the 3 semicircular canals, although the posterior canal is affected in >90% of cases ■ causes: head injury, viral infection (URTI), degenerative disease, idiopathic
■ results in slightly different signals being received by the brain from the two balance organs, resulting
in sensation of movement
Diagnosis
• history(timecourse,provokingfactors,associativesymptoms)
• positiveDix-Hallpikemaneuver(sensitivity82%,specificity71%)
Dix-Hallpike Positional Testing (see website for video and illustrations)
• thepatientisrapidlymovedfromasittingpositiontoasupinepositionwiththeheadhangingoverthe end of the table, turned to one side at 45°, and neck extended 20° holding the position for 20 s
• onsetofvertigoandrotarynystagmusindicateapositivetestforthedependentside
• other diagnostic testing is not indicated in posterior canal BPPV
Treatment
• reassurepatientthatprocessresolvesspontaneously • particlerepositioningmaneuvers
■ Epley maneuver (performed by MD or by patient with the help of devices such as the DizzyFIXTM)
■ Brandt-Daroff exercises (performed by patient)
• anti-emeticsforN/V
• surgeryforrefractorycases
• drugstosuppressthevestibularsystemdelayeventualrecoveryandarethereforenotused
Ménière’s Disease (Endolymphatic Hydrops)
Definition
• episodicattacksoftinnitus,hearingloss,auralfullness,andvertigolastingmintoh
Proposed Etiology
• inadequateabsorptionofendolymphleadstoendolymphatichydrops(overaccumulation)thatdistorts the membranous labyrinth
Epidemiology
• peakincidence40-60yr • bilateralin35%ofcases
BPPV is the most common cause of episodic vertigo; patients are often symptomatic when rolling over in bed or moving their head to a position of extreme posterior extension (such as looking up at a tall building or getting their hair washed at the hairdresser)
Signs of BPPV seen with Dix-Hallpike Maneuver
• Latency of ~20 s
• Crescendo/decrescendovertigolasting20s
• Geotropic rotatory nystagmus (nystagmus
MUST be present for a positive test)
• Reversal of nystagmus upon sitting up
• Fatigability with repeated stimulation
Diagnostic Criteria for Ménière’s Disease (must have all three)
• Two spontaneous episodes of rotational
vertigo ≥20 minutes
• Audiometric confirmation of SNHL (often
low frequency)
• Tinnitus and/or aural fullness
