
Page 1088 - TNFlipTest
P. 1088
P54 Pediatrics
Infectious Diseases Toronto Notes 2019
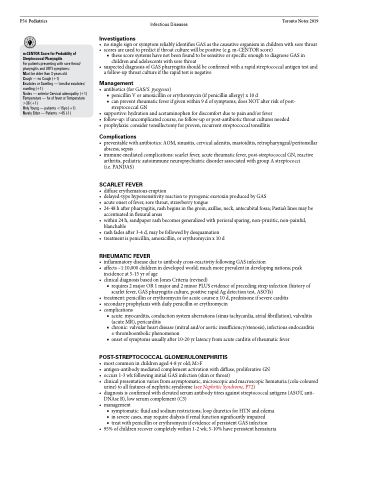
m-CENTOR Score for Probability of Streptococcal Pharyngitis
For patients presenting with sore throat/ pharyngitis and URTI symptoms:
Must be older than 3 years old
Cough — no Cough (+1)
Exudates or Swelling — tonsillar exudates/ swelling (+1)
Nodes — anterior Cervical adenopathy (+1) Temperature — hx of fever or Temperature >38 (+1)
Only Young — patients <15yo (+1)
Rarely Elder — Patients >45 (-1)
Investigations
• nosinglesignorsymptomreliablyidentifiesGASasthecausativeorganisminchildrenwithsorethroat
• scoresareusedtopredictifthroatculturewillbepositive(e.g.m-CENTORscore)
■ these score systems have not been found to be sensitive or specific enough to diagnose GAS in children and adolescents with sore throat
• suspecteddiagnosisofGASpharyngitisshouldbeconfirmedwitharapidstreptococcalantigentestand a follow-up throat culture if the rapid test is negative
Management
• antibiotics(forGAS/S.pyogenes)
■ penicillin V or amoxicillin or erythromycin (if penicillin allergy) x 10 d
■ can prevent rheumatic fever if given within 9 d of symptoms; does NOT alter risk of post-
streptococcal GN
• supportive:hydrationandacetaminophenfordiscomfortduetopainand/orfever
• follow-up:ifuncomplicatedcourse,nofollow-uporpost-antibioticthroatculturesneeded • prophylaxis:considertonsillectomyforproven,recurrentstreptococcaltonsillitis
Complications
• preventablewithantibiotics:AOM,sinusitis,cervicaladenitis,mastoiditis,retropharyngeal/peritonsillar abscess, sepsis
• immune-mediatedcomplications:scarletfever,acuterheumaticfever,post-streptococcalGN,reactive arthritis, pediatric autoimmune neuropsychiatric disorder associated with group A streptococci
(i.e. PANDAS)
SCARLET FEVER
• diffuseerythematouseruption
• delayed-typehypersensitivityreactiontopyrogenicexotoxinproducedbyGAS
• acuteonsetoffever,sorethroat,strawberrytongue
• 24-48hafterpharyngitis,rashbeginsinthegroin,axillae,neck,antecubitalfossa;Pastia’slinesmaybe
accentuated in flexural areas
• within24h,sandpaperrashbecomesgeneralizedwithperioralsparing,non-pruritic,non-painful,
blanchable
• rashfadesafter3-4d,maybefollowedbydesquamation
• treatmentispenicillin,amoxicillin,orerythromycinx10d
RHEUMATIC FEVER
• inflammatorydiseaseduetoantibodycross-reactivityfollowingGASinfection
• affects~1:10,000childrenindevelopedworld;muchmoreprevalentindevelopingnations;peak
incidence at 5-15 yr of age
• clinicaldiagnosisbasedonJonesCriteria(revised)
■ requires 2 major OR 1 major and 2 minor PLUS evidence of preceding strep infection (history of scarlet fever, GAS pharyngitis culture, positive rapid Ag detection test, ASOTs)
• treatment:penicillinorerythromycinforacutecoursex10d,prednisoneifseverecarditis
• secondaryprophylaxiswithdailypenicillinorerythromycin
• complications
■ acute: myocarditis, conduction system aberrations (sinus tachycardia, atrial fibrillation), valvulitis (acute MR), pericarditis
■ chronic: valvular heart disease (mitral and/or aortic insufficiency/stenosis), infectious endocarditis ± thromboembolic phenomenon
■ onset of symptoms usually after 10-20 yr latency from acute carditis of rheumatic fever
POST-STREPTOCOCCAL GLOMERULONEPHRITIS
• mostcommoninchildrenaged4-8yrold;M>F
• antigen-antibodymediatedcomplementactivationwithdiffuse,proliferativeGN
• occurs1-3wkfollowinginitialGASinfection(skinorthroat)
• clinicalpresentationvariesfromasymptomatic,microscopicandmacroscopichematuria(cola-coloured
urine) to all features of nephritic syndrome (see Nephritic Syndrome, P72)
• diagnosisisconfirmedwithelevatedserumantibodytitresagainststreptococcalantigens(ASOT,anti-
DNAse B), low serum complement (C3) • management
■ symptomatic: fluid and sodium restrictions; loop diuretics for HTN and edema ■ in severe cases, may require dialysis if renal function significantly impaired
■ treat with penicillin or erythromycin if evidence of persistent GAS infection
• 95%ofchildrenrecovercompletelywithin1-2wk;5-10%havepersistenthematuria
