
Page 1086 - TNFlipTest
P. 1086
P52 Pediatrics Infectious Diseases Toronto Notes 2019
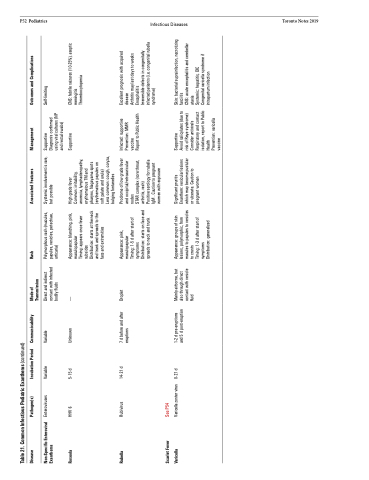
Table 21. Common Infectious Pediatric Exanthems (continued)
Disease
Pathogen(s)
Incubation Period Communicability
Mode of Transmission
Rash
Associated Features
Management
Outcomes and Complications
Non-Specific Enteroviral Exanthems
Enteroviruses
Variable
Variable
Direct and indirect contact with infected bodily fluids
Polymorphous rash (macules, papules, vesicles, petechiae, urticaria)
Systemic involvement is rare, but possible
Supportive
Diagnosis confirmed using viral cultures (NP and rectal swabs)
Self-limiting
Roseola
HHV 6
5-15 d
Unknown
—
Appearance: blanching, pink, maculopapular
Timing: appears once fever subsides
High grade fever
Common: irritability, anorexia, lymphadenopathy, erythematous TM and pharynx, Nagayama spots (erythematous papules on soft palate and uvula)
Less common: cough, coryza, bulging fontanelles
Supportive
CNS: febrile seizures (10-25%), aseptic meningitis
Thrombocytopenia
Rubella
Rubivirus
14-21 d
7 d before and after eruptions
Droplet
Appearance: pink, maculopapular
Timing: 1-5 d after start of symptoms
Prodrome of low grade fever and occipital/retroauricular nodes
STAR complex (sore throat, arthritis, rash)
Infected: supportive Prevention: MMR vaccine
Report to Public Health
Excellent prognosis with acquired disease
Arthritis may last days to weeks Encephalitis
Scarlet Fever Varicella
See P54
Varicella zoster virus
0-21 d
1-2 d pre-eruptions and 5 d post-eruption
Mainly airborne, but also through direct contact with vesicle fluid
Appearance: groups of skin lesions, polymorphic, from macules to papules to vesicles to crusts
Significant pruritis Enanthem: vesicular lesions which may become pustular or ulcerate. Caution to pregnant women
Supportive
Avoid salicylates (due to risk of Reye syndrome) Consider antivirals Respiratory and contact isolation, report to Public Health
Prevention: varicella vaccine
Skin: bacterial suprainfection, necrotizing fasciitis
CNS: acute encephalitis and cerebellar ataxia
Distribution: starts at the neck and trunk and spreads to the face and extremities
Distribution: starts on face and spreads to neck and trunk
Positive serology for rubella IgM . Caution to pregnant women with expsoure
Irreversible defects in congenitally infected patients (i.e. congenital rubella syndrome)
Timing: 1-3 d after start of symptoms
Distribution: generalized
Systemic: hepatitis, DIC Congenital varicella syndrome if intrapartum infection
