
Page 1146 - TNFlipTest
P. 1146
PL24 Plastic Surgery
High pressure injection injury, e.g. pain gun, is deceptively benign-looking (small pinpoint hole on finger pad) often with few clinical signs. Intense pain and tenderness, along
the course the foreign material travelled, is present a few hours after the injury. Definitive treatment is exposure and removal of foreign material
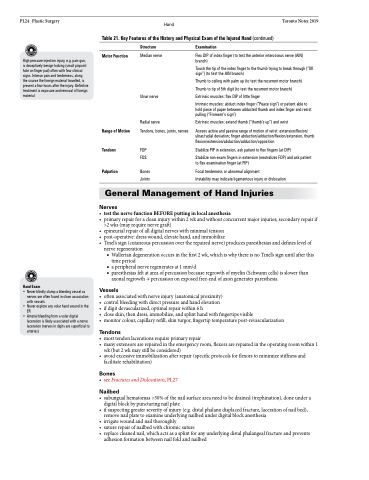
Hand Toronto Notes 2019 Table 21. Key Features of the History and Physical Exam of the Injured Hand (continued)
Motor Function
Range of Motion Tendons
Palpation
Structure
Median nerve
Ulnar nerve
Radial nerve
Tendons, bones, joints, nerves
FDP FDS
Bones Joints
Examination
Flex DIP of index finger (to test the anterior interosseus nerve (AIN) branch)
Touch the tip of the index finger to the thumb trying to break through (“OK sign”) (to test the AIN branch)
Thumb to ceiling with palm up (to test the recurrent motor branch) Thumb to tip of 5th digit (to test the recurrent motor branch) Extrinsic muscles: flex DIP of little finger
Intrinsic muscles: abduct index finger (“Peace sign”) or patient able to hold piece of paper between adducted thumb and index finger and resist pulling (“Froment’s sign”)
Extrinsic muscles: extend thumb (“thumb’s up”) and wrist
Assess active and passive range of motion of wrist: extension/flexion/ ulnar/radial deviation; finger abduction/adduction/flexion/extension, thumb flexion/extension/abduction/adduction/opposition
Stabilize PIP in extension, ask patient to flex fingers (at DIP)
Stabilize non-exam fingers in extension (neutralizes FDP) and ask patient to flex examination finger (at PIP)
Focal tenderness or abnormal alignment
Instability may indicate ligamentous injury or dislocation
Hand Exam
• Never blindly clamp a bleeding vessel as nerves are often found in close association with vessels
• Never explore any volar hand wound in the ER
• Arterial bleeding from a volar digital laceration is likely associated with a nerve laceration (nerves in digits are superficial to arteries)
General Management of Hand Injuries
Nerves
• testthenervefunctionBEFOREputtinginlocalanesthesia
• primaryrepairforacleaninjurywithin2wkandwithoutconcurrentmajorinjuries;secondaryrepairif
>2 wks (may require nerve graft)
• epineurialrepairofalldigitalnerveswithminimaltension
• post-operative:dresswound,elevatehand,andimmobilize
• Tinel’ssign(cutaneouspercussionovertherepairednerve)producesparesthesiasanddefineslevelof
nerve regeneration
■ Wallerian degeneration occurs in the first 2 wk, which is why there is no Tinel’s sign until after this
time period
■ a peripheral nerve regenerates at 1 mm/d
■ paresthesias felt at area of percussion because regrowth of myelin (Schwann cells) is slower than
axonal regrowth → percussion on exposed free-end of axon generates paresthesia
Vessels
• oftenassociatedwithnerveinjury(anatomicalproximity)
• controlbleedingwithdirectpressureandhandelevation
• ifdigitdevascularized,optimalrepairwithin6h
• closeskin,thendress,immobilize,andsplinthandwithfingertipsvisible
• monitorcolour,capillaryrefill,skinturgor,fingertiptemperaturepost-revascularization
Tendons
• mosttendonlacerationsrequireprimaryrepair
• manyextensorsarerepairedintheemergencyroom,flexorsarerepairedintheoperatingroomwithin1
wk (but 2 wk may still be considered)
• avoidexcessiveimmobilizationafterrepair(specificprotocolsforflexorstominimizestiffnessand
facilitate rehabilitation)
Bones
• seeFracturesandDislocations,PL27
Nailbed
• subungualhematomas>50%ofthenailsurfaceareaneedtobedrained(trephination),doneundera digital block by puncturing nail plate
• ifsuspectinggreaterseverityofinjury(e.g.distalphalanxdisplacedfracture,lacerationofnailbed), remove nail plate to examine underlying nailbed under digital block anesthesia
• irrigatewoundandnailthoroughly
• suturerepairofnailbedwithchromicsuture
• replacecleanednail,whichactsasasplintforanyunderlyingdistalphalangealfractureandprevents
adhesion formation between nail fold and nailbed
