
Page 1160 - TNFlipTest
P. 1160
PL38 Plastic Surgery
Breast
Toronto Notes 2019
Table 30. Alloplastic Reconstruction vs. Autogenous Reconstruction
A
B
C
D
E
F
Alloplastic Reconstruction
Autogenous Reconstruction
One stage reconstruction with implant
Two stage reconstruction with expander and implant
Latissimus Dorsi Flap
TRAM (Transverse Rectus Abdominis Muscle) Flap
DIEP (Deep Inferior Epigastric Perforator) Flap
Advantages
Shorter surgery
May give a more complete or final result
Less tension on mastectomy flaps compared to single-stage reconstruction with implants
Ability to increase skin to create breast and avoid use of flap
Some patient control over final outcome
Reliable pedicle
Uses patient’s own tissues
Provides skin and muscles
Possible to do muscle sparing procedure without flap compromise
Provides good amount of skin and muscle for reconstruction
Good option for delayed reconstruction, larger women, and to avoid complications of using abdominal wall
Can be done as a:
Fascial-sparing technique (Pedicled TRAM) Free tissue transfer (Free TRAM)
Provides a good amount of tissue for transfer in most women
Provides a well-concealed scar
Method spares rectus abdominis muscle and fascia and should theoretically preserve innervation and continuity of abdominal wall
Disadvantages
Size restriction in reconstruction Very few women meet criteria: grade 1 ptosis, small breast, skin-sparing mastectomy
Requires post-surgical procedures (requires patient to come to clinic for inflations)
Size of reconstruction limited to size and vascularity of mastectomy flaps
May also require implants for adequate volume
Second scar with second surgical site Volume depends on patient’s donor site
Pedicled TRAM:
Weakness in rectus abdominis with higher bulge rates
Free TRAM:
Similar complications to DIEPs
Less muscle used, decreased risk of hernia or bulge
Requires microsurgical training
for meticulous dissection of flap and appropriate choice of perforator
May not always be possible Abdominal scarring and second wound
Nipple Areolar Complex Reconstruction
• nipplereconstructionisusuallydoneasthefinalstepwhenthepatientissatisfiedwithbreastmound creation
• reconstruction can be performed with local anesthetic since many women have decreased sensation in the mastectomy or breast flaps
graft
• itcanbedonebyeitheraflap,graft,or3Dtattoo
Table 31. Types of Nipple Reconstruction
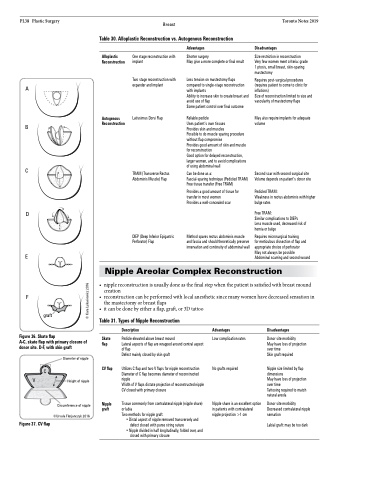
Figure 36. Skate flap
A-C, skate flap with primary closure of donor site. D-F, with skin graft
Skate flap
CV flap
Nipple graft
Description
Pedicle elevated above breast mound
Lateral aspects of flap are wrapped around central aspect of flap
Defect mainly closed by skin graft
Utilizes C flap and two V flaps for nipple reconstruction Diameter of C flap becomes diameter of reconstructed nipple
Width of V flaps dictate projection of reconstructed nipple CV closed with primary closure
Tissue commonly from contralateral nipple (nipple share) or labia
Two methods for nipple graft:
• Distal aspect of nipple removed transversely and defect closed with purse string suture
• Nipple divided in half longitudinally, folded over, and closed with primary closure
Advantages
Low complication rates
No grafts required
Nipple share is an excellent option in patients with contralateral nipple projection >1 cm
Disadvantages
Donor site morbidity
May have loss of projection over time
Skin graft required
Nipple size limited by flap dimensions
May have loss of projection over time
Tattooing required to match natural areola
Donor site morbidity Decreased contralateral nipple sensation
Labial graft: may be too dark
Diameter of nipple C
Height of nipple
Circumference of nipple
©Ursula Florjanczyk 2016
V
Figure 37. CV flap
© Kara Lukasiewicz 2016
