
Page 1199 - TNFlipTest
P. 1199
Toronto Notes 2019 Child Psychiatry Psychiatry PS35 Table 10. Description and Diagnosis of Personality Disorders (continued)
Cluster C “Sad” Personality Disorders
• Patients seem anxious, fearful
• Familial association with anxiety disorder
• Common defense mechanisms: isolation, avoidance, hypochondriasis
Avoidant Personality Disorder (0.5-1.6%)
Timid and socially awkward with a pervasive sense of inadequacy and fear of criticism. Fear of embarrassing or humiliating themselves in social situations so remain withdrawn and socially inhibited
Diagnosis requires 4+ of: CRINGES
1. Criticism or rejection preoccupies thoughts in social situations 2. Restraint in relationships due to fear of being shamed
3. Inhibited in new relationships due to fear of inadequacy
4. Needs to be sure of being liked before engaging socially
5. Gets around occupational activities requiring interpersonal contact 6. Embarrassment prevents new activity or taking risks
7. Self-viewed as unappealing or inferior
Dependent Personality Disorder (1.6-6.7%)
Pervasive and excessive need to be taken care of, excessive fear of separation, clinging and submissive behaviours. Difficulty making everyday decisions. Useful to set regulated treatment schedule (regular, brief visits) and being firm about in between issues. Encourage patient to do more for themselves, engage in own problem-solving
Diagnosis requires 5 of: RELIANCE
1. Reassurance required for everyday decisions
2. Expressing disagreement difficult
3. Life responsibilities assumed by others
4. Initiating projects difficult (because no confidence) 5. Alone (feels helpless and uncomfortable when alone) 6. Nurturance (goes to excessive lengths to obtain)
7. Companionship sought urgently
8. Exaggerated fears of being left to care for self
Table 11. Key Differences Among Schizoid, Schizotypal, and Schizophrenia
Obsessive-Compulsive Personality Disorder (3-10%)
Preoccupation with orderliness, perfectionism, and mental and interpersonal control. Is inflexible, closed-off, and inefficient
Diagnosis requires 4+ of: SCRIMPER
1. Stubborn
2. Cannot discard worthless objects
3. Rule/detail obsessed (to point of activity lost) 4. Inflexible in matters of morality, ethics, values 5. Miserly
6. Perfectionistic
7. Excludes leisure due to devotion to work
8. Reluctant to delegate to others
Thought Form Thought Content
Relationships
Schizoid
Organized
No psychosis
Solitary, NO desire for social relationships
Schizotypal
Organized, but vague and circumstantial
No psychosis, may have ideas of reference, paranoid ideation, odd beliefs and magical thinking
Lacks close relationships, INTERESTED in relationships but socially inept
Schizophrenia
Disorganized, tangential, loosening of associations
Psychosis, hallucinations
Socially marginalized, but not by choice
OCPD vs. OCD
Child Psychiatry
Developmental Concepts
Ego- Syntonic or Ego- Dystonic Thought Content
OCPD
Ego-syntonic
Obsessional thinking, no compulsions, strict routine and rigidity
in day-to-day matters,more perfectionistic and rigid
OCD
Ego-dystonic
Obsessions and compulsions, rituals, anxiety provoking unwanted intrusive thoughts
• temperament:achild’sinnatepsycho-physiologicalandbehaviouralcharacteristics(e.g.emotionality, activity, and sociability); spectrum from “difficult” to “slow-to-warm-up” to “easy temperament”
• parentalfit:thecongruencebetweenparentingstyle(authoritative,permissive)andchild’s temperament
• attachment:specialrelationshipbetweenchildandprimarycaretaker(s);developsduringfirstyear,the caretaker’s attachment style is the best predictor of their child’s attachment style, refer to Table 12
• separationanxiety(normalbetween10-18mo):whereseparationfromattachmentfigureresultsin distress
Consider speaking to children alone. Always consider child abuse. See Pediatrics, P14
Tips for the Child Interview
• Use language the child will understand (i.e. don’t ask about feeling of worthlessness, ask about whether they feel like they’re a bad kid)
• Children in some cultures are taught to be quiet and avoid eye contact with adults who are authority figures (do not mistake with depression)
• Use developmentally-appropriate questions (i.e. don’t ask about lack of interest in activities, ask children whether they feel bored)
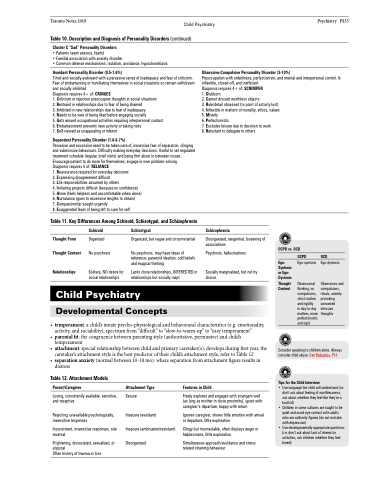
Table 12. Attachment Models
Parent/Caregiver
Loving, consistently available, sensitive, and receptive
Rejecting, unavailable psychologically, insensitive responses
Inconsistent, insensitive responses, role reversal
Frightening, dissociated, sexualized, or atypical
Often history of trauma or loss
Attachment Type
Secure
Insecure (avoidant)
Insecure (ambivalent/resistant) Disorganized
Features in Child
Freely explores and engages with strangers well (as long as mother in close proximity), upset with caregiver’s departure, happy with return
Ignores caregiver, shows little emotion with arrival or departure, little exploration
Clingy but inconsolable, often displays anger or helplessness, little exploration
Simultaneous approach/avoidance and stress related straining behaviour
