
Page 1263 - TNFlipTest
P. 1263
Toronto Notes 2019 Pulmonary Vascular Disease Pulmonary Vascular Disease
Pulmonary Hypertension
Definition
• meanpulmonaryarterialpressure>25mmHgatrestand>30mmHgwithexercise,orasystolic pulmonary artery pressure of >40 mmHg at rest
Respirology R17
• pulmonaryHTNisgroupedinto5categoriesandclassifiedbasedonetiology
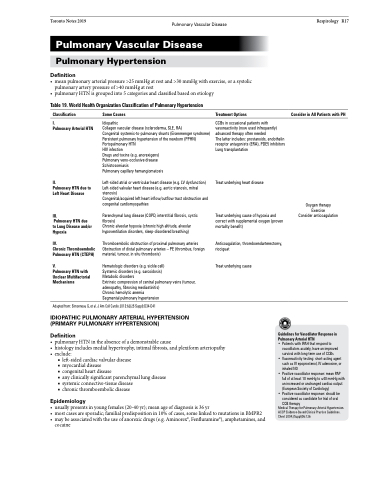
Table 19. World Health Organization Classification of Pulmonary Hypertension
Classification
I.
Pulmonary Arterial HTN
II.
Pulmonary HTN due to Left Heart Disease
III.
Pulmonary HTN due
to Lung Disease and/or Hypoxia
IV.
Chronic Thromboembolic Pulmonary HTN (CTEPH)
V.
Pulmonary HTN with Unclear Multifactorial Mechanisms
Some Causes
Idiopathic
Collagen vascular disease (scleroderma, SLE, RA)
Congenital systemic-to-pulmonary shunts (Eisenmenger syndrome) Persistent pulmonary hypertension of the newborn (PPHN) Portopulmonary HTN
HIV infection
Drugs and toxins (e.g. anorexigens)
Pulmonary veno-occlusive disease
Schistosomiasis
Pulmonary capillary hemangiomatosis
Left-sided atrial or ventricular heart disease (e.g. LV dysfunction) Left-sided valvular heart disease (e.g. aortic stenosis, mitral stenosis)
Congenital/acquired left heart inflow/outflow tract obstruction and congenital cardiomyopathies
Parenchymal lung disease (COPD, interstitial fibrosis, cystic fibrosis)
Chronic alveolar hypoxia (chronic high altitude, alveolar hypoventilation disorders, sleep-disordered breathing)
Thromboembolic obstruction of proximal pulmonary arteries Obstruction of distal pulmonary arteries – PE (thrombus, foreign material, tumour, in situ thrombosis)
Hematologic disorders (e.g. sickle cell)
Systemic disorders (e.g. sarcoidosis)
Metabolic disorders
Extrinsic compression of central pulmonary veins (tumour, adenopathy, fibrosing mediastinitis)
Chronic hemolytic anemia Segmental pulmonary hypertension
Treatment Options
CCBs in occasional patients with vasoreactivity (now used infrequently) advanced therapy often needed
The latter includes: prostanoids, endothelin receptor antagonists (ERA), PDE5 inhibitors Lung transplantation
Treat underlying heart disease
Treat underlying cause of hypoxia and correct with supplemental oxygen (proven mortality benefit)
Anticoagulation, thromboendarterectomy, riociguat
Treat underlying cause
Consider in All Patients with PH
Adapted from: Simonneau G, et al. J Am Coll Cardio 2013:62(25 Suppl):D34-D41
IDIOPATHIC PULMONARY ARTERIAL HYPERTENSION (PRIMARY PULMONARY HYPERTENSION)
Definition
Guidelines for Vasodilator Response in Pulmonary Arterial HTN
• Patients with IPAH that respond to
vasodilators acutely, have an improved
survival with long-term use of CCBs
• Vasoreactivity testing: short-acting agent such as IV epoprostenol, IV adenosine, or
inhaled NO
• Positive vasodilator response: mean PAP
fall of at least 10 mmHg to ≤40 mmHg with an increased or unchanged cardiac output (European Society of Cardiology)
• Positive vasodilator response: should be considered as candidate for trial of oral CCB therapy
Medical Therapy for Pulmonary Arterial Hypertension. ACCP Evidence-Based Clinical Practice Guidelines. Chest 2004;(Suppl)06:126
Oxygen therapy Exercise Consider anticoagulation
• pulmonaryHTNintheabsenceofademonstrablecause
• histologyincludesmedialhypertrophy,intimalfibrosis,andplexiformarteriopathy • exclude:
■ left-sided cardiac valvular disease
■ myocardial disease
■ congenital heart disease
■ any clinically significant parenchymal lung disease ■ systemic connective-tissue disease
■ chronic thromboembolic disease
Epidemiology
• usuallypresentsinyoungfemales(20-40yr);meanageofdiagnosisis36yr
• mostcasesaresporadic;familialpredispositionin10%ofcases,somelinkedtomutationsinBMPR2
• maybeassociatedwiththeuseofanorexicdrugs(e.g.Aminorex®,Fenfluramine®),amphetamines,and
cocaine
