
Page 148 - TNFlipTest
P. 148
D14 Dermatology
Dermatitis (Eczema) Toronto Notes 2019
■ topical calcineurin inhibitors
◆ tacrolimus 0.03%, 0.1% (Protopic®) and pimecrolimus 1% (Elidel®)
◆ use as steroid-sparing agents in the long-term
◆ advantages over long-term corticosteroid use: sustained effect in controlling pruritus; no skin
atrophy; safe for the face and neck
◆ apply 2x/d for acute flares, and 2-3x/wk to recurrent sites to prevent relapses
◆ local side effects: stinging, burning, allergic contact dermatitis
◆ U.S. black box warning of malignancy risk: rare cases of skin cancer and lymphoma reported;
no causal relationship established, warning is discounted by both the Canadian Dermatology Association and the American Academy of Dermatology
Complications
• infections
■ treatment of infections
■ topical mupirocin, retapamulin, ozenoxacin or fusidic acid (Canada only, not available in US) ■ oral antibiotics (e.g. cloxacillin, cephalexin) for widespread S. aureus infections
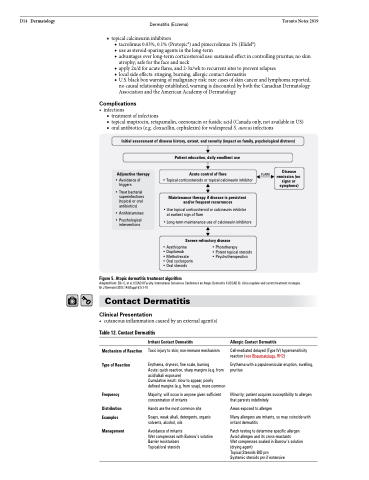
Initial assessment of disease history, extent, and severity (impact on family, psychological distress) Patient education, daily emollient use
Adjunctive therapy
• Avoidance of triggers
• Treat bacterial superinfections (topical or oral antibiotics)
• Antihistamines
• Psychological interventions
Acute control of flare
• Topical corticosteroids or topical calcineurin inhibitor
Maintenance therapy if disease is persistent and/or frequent recurrences
• Use topical corticosteroid or calcineurin inhibitor at earliest sign of flare
• Long-term maintenance use of calcineurin inhibitors
Severe refractory disease
FLARE
Disease remission (no signs or symptoms)
Figure 5. Atopic dermatitis treatment algorithm
• Azathioprine
• Dupilumab
• Methotrexate
• Oral cyclosporin
• Oral steroids
• Phototherapy
• Potent topical steroids • Psychotherapeutics
Adapted from: Ellis C, et al. ICCAD II Faculty. International Consensus Conference on Atopic Dermatitis II (ICCAD II): clinical update and current treatment strategies. Br J Dermatol 2003;148(Suppl 63):3-10
Contact Dermatitis
Clinical Presentation
• cutaneousinflammationcausedbyanexternalagent(s)
Table 12. Contact Dermatitis
Mechanism of Reaction
Type of Reaction
Frequency
Distribution Examples
Management
Irritant Contact Dermatitis
Toxic injury to skin; non-immune mechanism
Erythema, dryness, fine scale, burning
Acute: quick reaction, sharp margins (e.g. from acid/alkali exposure)
Cumulative insult: slow to appear, poorly defined margins (e.g. from soap), more common
Majority; will occur in anyone given sufficient concentration of irritants
Hands are the most common site
Soaps, weak alkali, detergents, organic solvents, alcohol, oils
Avoidance of irritants
Wet compresses with Burrow’s solution Barrier moisturizers
Topical/oral steroids
Allergic Contact Dermatitis
Cell-mediated delayed (Type IV) hypersensitivity reaction (see Rheumatology, RH2)
Erythema with a papulovesicular eruption, swelling, pruritus
Minority; patient acquires susceptibility to allergen that persists indefinitely
Areas exposed to allergen
Many allergens are irritants, so may coincide with irritant dermatitis
Patch testing to determine specific allergen Avoid allergen and its cross-reactants
Wet compresses soaked in Burrow’s solution (drying agent)
Topical Steroids BID prn Systemic steroids prn if extensive
