
Page 200 - TNFlipTest
P. 200
ER20 Emergency Medicine
Approach to Common ED Presentations
Toronto Notes 2019
Possible Causes of Coma
AEIOU TIPS
Acidosis/Alcohol
Epilepsy
Infection
Oxygen (hypoxia)/Opiates
Uremia
Temperature/Trauma (especially head) Insulin (too little or too much) Psychogenic/Poisoning
Stroke
(Majority) Toxic/Metabolic
Major organ failure Electrolyte/Endocrine Toxins/Temperature Acid disorders
Base disorders decreased Oxygen level Lactate
Insulin/Infection (sepsis) Cardiac/hyperCalcemia
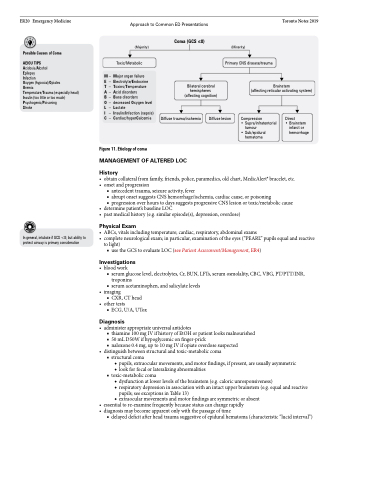
Coma (GCS ≤8)
Bilateral cerebral hemispheres (affecting cognition)
(Minority)
Primary CNS disease/trauma
M – E – T – A – B – O – L – I – C –
Brainstem
(affecting reticular activating system)
Figure 11. Etiology of coma
MANAGEMENT OF ALTERED LOC
History
Diffuse trauma/ischemia
Diffuse lesion
Compression
• Supra/infratentorial
tumour
• Sub/epidural
hematoma
Direct
• Brainstem
infarct or hemorrhage
In general, intubate if GCS <8; but ability to protect airway is primary consideration
• obtaincollateralfromfamily,friends,police,paramedics,oldchart,MedicAlert®bracelet,etc. • onsetandprogression
■ antecedent trauma, seizure activity, fever
■ abrupt onset suggests CNS hemorrhage/ischemia, cardiac cause, or poisoning
■ progression over hours to days suggests progressive CNS lesion or toxic/metabolic cause
• determinepatient’sbaselineLOC
• pastmedicalhistory(e.g.similarepisode(s),depression,overdose)
Physical Exam
• ABCs,vitalsincludingtemperature;cardiac,respiratory,abdominalexams
• completeneurologicalexam;inparticular,examinationoftheeyes(“PEARL”pupilsequalandreactive
to light)
■ use the GCS to evaluate LOC (see Patient Assessment/Management, ER4)
Investigations
• bloodwork
■ serum glucose level, electrolytes, Cr, BUN, LFTs, serum osmolality, CBC, VBG, PT/PTT/INR,
troponins
■ serum acetaminophen, and salicylate levels
• imaging
■ CXR, CT head
• othertests
■ ECG, U/A, UTox
Diagnosis
• administerappropriateuniversalantidotes
■ thiamine 100 mg IV if history of EtOH or patient looks malnourished ■ 50mLD50Wifhypoglycemiconfinger-prick
■ naloxone 0.4 mg, up to 10 mg IV if opiate overdose suspected
• distinguishbetweenstructuralandtoxic-metaboliccoma ■ structural coma
◆ pupils, extraocular movements, and motor findings, if present, are usually asymmetric
◆ look for focal or lateralizing abnormalities ■ toxic-metabolic coma
◆ dysfunction at lower levels of the brainstem (e.g. caloric unresponsiveness)
◆ respiratory depression in association with an intact upper brainstem (e.g. equal and reactive
pupils; see exceptions in Table 13)
◆ extraocular movements and motor findings are symmetric or absent
• essentialtore-examinefrequentlybecausestatuscanchangerapidly • diagnosismaybecomeapparentonlywiththepassageoftime
■ delayed deficit after head trauma suggestive of epidural hematoma (characteristic “lucid interval”)
