
Page 202 - TNFlipTest
P. 202
ER22 Emergency Medicine
Approach to Common ED Presentations
Toronto Notes 2019
ACS more likely to be atypical in females, diabetics, and >80 yr. Anginal equivalents include dyspnea, diaphoresis, fatigue, non- retrosternal pain
Signs of PE on CXR
Westermark’s sign: abrupt tapering of a vessel on chest film
Hampton’s hump: a wedge-shaped infiltrate that abuts the pleura
Effusion, atelectasis, or infiltrates 50% normal
It is important to look for reciprocal changes in STEMI in order to differentiate from pericarditis (diffuse elevations)
Tracheal deviation is away from tension or towards non-tension pneumothorax
Addition of Clopidogrel to Aspirin® and Fibrinolytic Therapy for Myocardial Infarction with ST-Segment Elevation
NEJM 2005;352:1179-91
Purpose: To assess the benefit of adding clopidogrel to Aspirin® and fibrinolytic therapy in ST-elevation MI.
Methods: Double-blind, RCT of Individuals presenting within 12 h of onset of ST-elevation
MI, comparing clopidogrel (300 mg loading dose followed by 75 mg OD until day of angiogram) versus placebo, in addition to Aspirin®, a fibrinolytic agent, and heparin when appropriate. Primary outcome was composite of occluded infarct-related artery on angiography (thrombosis in MI flow grade 0 or 1), or death or recurrent MI prior to angiography. Follow-up was at 30 days. Analysis was by intention to treat.
Results: 3,491 patients were included (mean age 57, 80.3% male, 50.3% smokers, 9.1% previous MI). Rates of the primary endpoint were 21.7% in the placebo group and 15.0% in the clopidogrel group (95% CI 24-47%). Among the individual components of the primary endpoint, clopidigrel had a significant effect on the rate of an occluded infarct-related artery and the rate of recurrent MI, but no effect on the rate of death from any cause. At 30 d clinical follow-up, there was no difference in rate of death from cardiovascular causes, a significant reduction in the odds of recurrent MI, and a non-significant reduction in recurrent ischemia with need for urgent revascularization. The rates of major bleeding and intracranial hemorrhage were similar between the two groups.
Conclusion: Addition of clopidogrel improves
the patency rate of infarct-related arteries and reduces ischemic complications, both of which are associated with improved long-term survival after MI. The trial was not powered to detect a survival benefit, and none was seen.
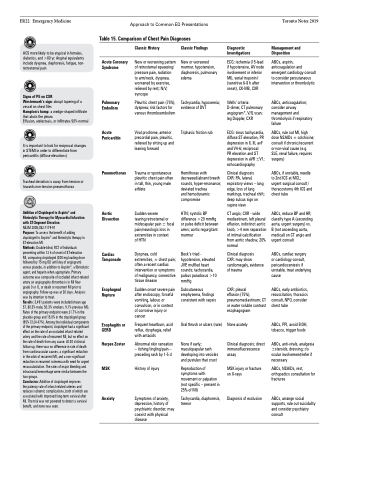
Acute Coronary Syndrome
Pulmonary Embolism
Acute Pericarditis
Pneumothorax
Aortic Dissection
Cardiac Tamponade
Esophageal Rupture
Esophagitis or GERD
Herpes Zoster
MSK
Anxiety
Classic History
New or worsening pattern of retrosternal squeezing/ pressure pain, radiation to arm/neck, dyspnea, worsened by exercise, relieved by rest; N/V; syncope
Pleuritic chest pain (75%), dyspnea; risk factors for venous thromboembolism
Viral prodrome, anterior precordial pain, pleuritic, relieved by sitting up and leaning forward
Trauma or spontaneous pleuritic chest pain often in tall, thin, young male athlete
Sudden severe
tearing retrosternal or midscapular pain ± focal pain/neurologic loss in extremities in context
of HTN
Dyspnea, cold extremities, ± chest pain; often a recent cardiac intervention or symptoms of malignancy, connective tissue disease
Sudden onset severe pain after endoscopy, forceful vomiting, labour, or convulsion, or in context of corrosive injury or cancer
Frequent heartburn, acid reflux, dysphagia, relief with antacids
Abnormal skin sensation – itching/tingling/pain – preceding rash by 1-5 d
History of injury
Symptoms of anxiety, depression, history of psychiatric disorder; may coexist with physical disease
Classic Findings
New or worsened murmur, hypotension, diaphoresis, pulmonary edema
Tachycardia, hypoxemia; evidence of DVT
Triphasic friction rub
Hemithorax with decreased/absent breath sounds, hyper-resonance; deviated trachea
and hemodynamic compromise
HTN; systolic BP difference >20 mmHg or pulse deficit between arms; aortic regurgitant murmur
Beck’s triad - hypotension, elevated JVP, muffled heart sounds; tachycardia, pulsus paradoxus >10 mmHg
Subcutaneous emphysema, findings consistent with sepsis
Oral thrush or ulcers (rare)
None if early; maculopapular rash developing into vesicles and pustules that crust
Reproduction of symptoms with movement or palpation (not specific – present in 25% of MI)
Tachycardia, diaphoresis, tremor
Diagnostic Investigations
ECG: ischemia (15-lead if hypotensive, AV node involvement or inferior MI), serial troponin I (sensitive 6-8 h after onset), CK-MB, CXR
Wells’ criteria: D-dimer, CT pulmonary angiogram*, V/Q scan; leg Doppler, CXR
ECG: sinus tachycardia, diffuse ST elevation, PR depression in II, III, avF and V4-6; reciprocal
PR elevation and ST depression in aVR ±V1; echocardiography
Clinical diagnosis
CXR: PA, lateral, expiratory views – lung edge, loss of lung markings, tracheal shift; deep sulcus sign on supine view
CT angio; CXR - wide mediastinum, left pleural effusion, indistinct aortic knob, >4 mm separation of intimal calcification from aortic shadow, 20% normal
Clinical diagnosis
CXR: may show cardiomegaly, evidence of trauma
CXR: pleural
effusion (75%), pneumomediastinum; CT or water soluble contrast esophagogram
None acutely
Clinical diagnosis; direct immunofluorescence assay
MSK injury or fracture on X-rays
Diagnosis of exclusion
Management and Disposition
ABCs, aspirin, anticoagulation and emergent cardiology consult to consider percutaneous intervention or thrombolytic
ABCs, anticoagulation; consider airway management and thrombolysis if respiratory failure
ABCs, rule out MI, high dose NSAIDs ± colchicine; consult if chronic/recurrent or non-viral cause (e.g. SLE, renal failure, requires surgery)
ABCs, if unstable, needle to 2nd ICS at MCL; urgent surgical consult / thoracostomy 4th ICS and chest tube
ABCs, reduce BP and HR; classify type A (ascending aorta, urgent surgery) vs. B (not ascending aorta, medical) on CT angio and urgent consult
ABCs, cardiac surgery
or cardiology consult, pericardiocentesis if unstable, treat underlying cause
ABCs, early antibiotics, resuscitation, thoracics consult, NPO, consider chest tube
ABCs, PPI, avoid EtOH, tobacco, trigger foods
ABCs, anti-virals, analgesia ±steroids, dressing; r/o ocular involvement/refer if necessary
ABCs, NSAIDs, rest, orthopedics consultation for fractures
ABCs, arrange social supports, rule out suicidality and consider psychiatry consult
Table 15. Comparison of Chest Pain Diagnoses
