
Page 306 - TNFlipTest
P. 306
FM8 Family Medicine
Health Promotion and Counselling Toronto Notes 2019
Screening Recommendations
• CANRISKorFINRISCscorescanbeusedtoassesstheriskfortype2DMinoverweightandobese patients
• recommendsmeasuringheightandweightandthencalculatingBMIatappropriateprimarycarevisits
Management
Behavioural/ Lifestyle
• weightlossof>5%isclinicallysignificantforreducingmanycardiovascularriskfactors(e.g.elevated blood pressure, glucose, and lipids)
• efficacious behavioural interventions: >12 months duration, include diet, exercise, lifestyle components, and group and individual sessions
• structuredbehaviouralandlifestyleinterventionsshouldbeofferedorarrangedforoverweight individuals BMI >25
• strongrecommendationforthosewithincreasedriskofType2DM
• BMI>35andriskfactorsorBMI>40arecandidatesforbariatricsurgeryfailingbehavioural
modification
Pharmacologic
• recommendsagainstpharmacologicinterventiontomanagepatientswhoareoverweightandobese, although some patients may prefer medications and be good candidates for pharmacologic treatment
• highbenefitofbehaviouralmodificationalone,NNH(numberneededtoharm)10(mostlyGIside effects) for pharmacotherapy
Pharmacotherapy for Obesity
• Orlistat: gastrointestinal lipase inhibitor, reduces fat absorption by 30% by inhibition of pancreatic lipase
• Orlistat is associated with several adverse effects and not approved for clinical use longer than 2 yr
• Orlistat should be avoided in people with inflammatory or chronic bowel disease
“TheLatestEvidenceonFadDiets...” - Comparison of the Atkins, Ornish, Weight Watchers, and Zone Diets for Weight Loss and Heart Disease Risk Reduction
JAMA 2005;293:43-53
Purpose: To assess the effectiveness and adherence rates of four popular diets for weight loss and reduction of cardiac risk factors.
Methods: SinglecentreRCTatacademicmedical centre in Boston, MA. Participants were randomized to either Atkins (carbohydrate restriction), Zone (macronutrient balanced and low glycemic load), Weight Watchers (low calorie/portion size), or Ornish (fat restriction) diet groups for a period of 18 mo. Participants were adults aged 22-72 years with known HTN, dyslipidemia, or fasting hyperglycemia. Results: 160 participants were randomized. Assuming that participants who discontinued the study remained at baseline, the mean weight loss at 1 yr (and self selected dietary adherence rates per self report) were 2.1 kg for Atkins (53% of participants completed, p=0.009), 3.2 kg for the Zone (65% of participants completed, p=0.002), 3.0 kg for Weight Watchers (65% completed, p<0.001), 3.3 kg for Ornish (50% completed, p=0.007). Each diet significantly reduced the LDL/ HDL ratio by ~10% (p<0.05), with no significant effects on blood pressure or glucose. Amount of weight loss was associated with adherence level
(r = 0.60; p<0.001) but not with diet type (r = 0.07; p=0 .40). Weight loss for each diet was significantly associated with reduction in levels of total/HDL cholesterol (r=0.36), C-reactive protein (r=0.37), and insulin (r=0.39), with no significant difference between diets.
Conclusion: Each popular diet was associated with modest weight loss and reduction of several cardiac risk factors. Adherence level, and not diet type, was the most important predictor of weight loss and cardiac risk factor reduction.
Hyperlipidemia Signs
• Atheromata: plaques in blood vessel walls
• Xanthelasmata: a sharply demarcated
yellowish deposit of cholesterol underneath
the skin, usually on or around the eyelid
• Tendinous xanthoma: lipid deposit in
tendon (especially Achilles)
• Eruptive xanthoma: hypertriglyceridemia
induced reddish yellow, pruritic, and painful
papular or nodular rash
• Lipemia retinalis: thin atheromata seen in
the retinal blood vessels
• Corneal arcus (arcus senilis): lipid deposit
in cornea
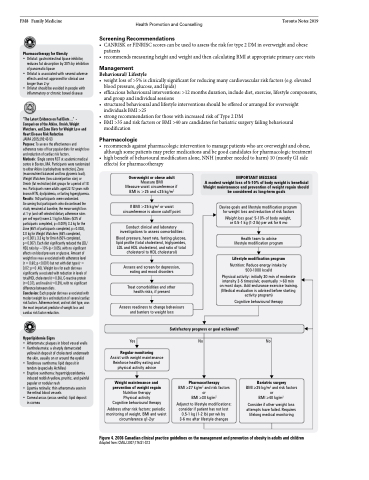
Overweight or obese adult
Measure BMI Measure waist circumference if BMI is >25 and ≤35 kg/m2
If BMI >25 kg/m2 or waist circumference is above cutoff point
Conduct clinical and laboratory investigations to assess comorbidities:
Blood pressure, heart rate, fasting glucose, lipid profile (total cholesterol, triglycerides, LDL and HDL cholesterol, and ratio of total cholesterol to HDL cholesterol)
Assess and screen for depression, eating and mood disorders
Treat comorbidities and other health risks, if present
Assess readiness to change behaviours and barriers to weight loss
IMPORTANT MESSAGE
A modest weight loss of 5-10% of body weight is beneficial Weight maintenance and prevention of weight regain should be considered as long-term goals
Devise goals and lifestyle modification program for weight loss and reduction of risk factors
Weight loss goal: 5-10% of body weight, or 0.5-1 kg (1-2 lb) per wk for 6 mo
Health team to advise lifestyle modification program
Lifestyle modification program
Nutrition: Reduce energy intake by 500-1000 kcal/d
Physical activity: initially 30 min of moderate
intensity 3-5 times/wk; eventually >60 min on most days. Add endurance exercise training. (Medical evaluation is advised before starting activity program)
Cognitive behavioural therapy
Yes
Regular monitoring
Assist with weight maintenance Reinforce healthy eating and physical activity advice
Weight maintenance and prevention of weight regain Nutrition therapy Physical activity Cognitive behavioural therapy
Address other risk factors: periodic monitoring of weight, BMI and waist circumference q1-2yr
Satisfactory progress or goal achieved?
No
Pharmacotherapy
BMI ≥27 kg/m2 and risk factors or
BMI ≥30 kg/m2
Adjunct to lifestyle modifications: consider if patient has not lost 0.5-1 kg (1-2 lb) per wk by 3-6 mo after lifestyle changes
No
Bariatric surgery
BMI ≥35 kg/m2 and risk factors or
BMI ≥40 kg/m2
Consider if other weight loss attempts have failed. Requires lifelong medical monitoring
Figure 4. 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children
Adapted from: CMAJ 2007;176:S1-S13
