
Page 307 - TNFlipTest
P. 307
Toronto Notes 2019 Health Promotion and Counselling Dyslipidemia
• seeEndocrinology,E2
• definedasabnormalelevationofplasmacholesterolortriglyceridelevels
Family Medicine FM9
To calculate Framingham Risk Score, go
to http://www.framinghamheartstudy.org/ risk-functions/cardiovascular-disease/10-year- risk.php#
Risk Factors for Screening for Dyslipidemia
• First Nations or South Asian ancestry • Current cigarette smoking
• Diabetes
• Arterial Hypertension
• Family history of premature CVD • Family history of hyperlipidemia • Erectile dysfunction
• Chronic kidney disease
• Inflammatory disease (lupus, rheumatoid arthritis, psoriatic arthritis, IBD)
• HIV infection
• Chronic obstructive pulmonary disease • Clinical evidence of atherosclerosis or
abdominal aneurysm
• Clinical manifestation of hyperlipidemia • Obesity (BMI>27)
Non-fasting Lipids vs. Fasting Lipids
Non-fasting (TC and non-HDL cholesterol) can be used for Framingham Risk Assessment and hold same prognostic value as fasting lipids
In fasted vs. non-fasted samples, non-HDL and TC varies by 2%, LDL-C by 10% and TG
by 20%
Recently, non-fasting LDL-C has the same prognostic value as fasting LDL-C
Ontario Association of Medical Laboratories Guidelines for Lipid Testing in Adults (2013): http:// www.oaml.com/documents/elineforAdultLipidTest- ingFinal2013_000.pdf
LDL cannot be calculated when TG ≥4.5 mmol/L
Safety of Statins: An Update
Therapeutic Advances in Drug Safety 2012;3:133-144 Trials have shown that statin therapy slightly increases the incidence of diabetes; however, the absolute risk is small. Relative to the reduction in coronary events, the clinical significance is not great enough to recommend against their use.
Use with caution when prescribing combined statin and fibrate therapy as there has been concern regarding the safety of certain combinations (potential increased risk of myopathy and rhabdomyolysis)
Assessment
No Pharmacology Low Risk
FRS <10%
1. Smoking cessation
YES
Monitor
Response to statin Rx Health behaviour
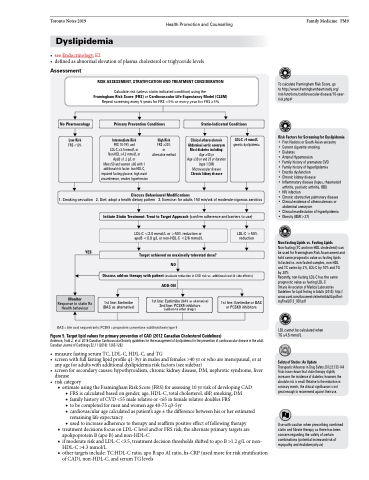
RISK ASSESSMENT, STRATIFICATION AND TREATMENT CONSIDERATION
Calculate risk (unless statin-indicated condition) using the Framingham Risk Score (FRS) or Cardiovascular Life Expectancy Model (CLEM) Repeat screening every 5 years for FRS <5% or every year for FRS ≥5%
Primary Prevention Conditions
Statin-Indicated Conditions
Intermediate Risk
FRS 10-19% and
LDL-C ≥3.5 mmol/L or Non-HDL ≥4.3 mmol/L or ApoB ≥1.2 g/L or
Men≥50 and women ≥60 with 1 additional risk factor: low HDL-C, impaired fasting glucose, high waist circumference, smoker, hypertension
High Risk
FRS ≥20%
or alternative method
Clinical atherosclerosis Abdominal aortic aneurysm Most diabetes including: Age ≥40 yr
Age ≥30 yr and 25 yr duration (type 1 DM) Microvascular disease Chronic kidney disease
LDL-C ≥5 mmol/L genetic dyslipidemia
Discuss Behavioural Modifications
2. Diet: adopt a health dietary pattern 3. Exercise: for adults 150 min/wk of moderate-vigorous aerobics
Initiate Statin Treatment: Treat to Target Approach (confirm adherence and barriers to use)
LDL-C <2.0 mmol/L or >50% reduction or apoB <0.8 g/L or non-HDL-C <2/6 mmol/L
Target achieved on maximally tolerated dose? NO
LDL-C >50% reduction
Discuss add-on therapy with patient (evaluate reduction in CVD risk vs. additional cost & side effects) ADD-ON
1st line: Ezetimibe (BAS as alternative)
1st line: Ezetimibe (BAS as alternative) 2nd line: PCSK9 inhibitors (add-on to other drugs)
1st line: Ezetimibe or BAS or PCSK9 inhibitors
BAS = bile acid sequestrants; PCSK9 = proprotein convertase subtilisin/kexin type 9
Figure 5. Target lipid values for primary prevention of CAD (2012 Canadian Cholesterol Guidelines)
Anderson, Todd J., et al. 2016 Canadian Cardiovascular Society guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in the adult. Canadian Journal of Cardiology 32.11 (2016): 1263-1282
• measurefastingserumTC,LDL-C,HDL-C,andTG
• screenwithfullfastinglipidprofileq1-3yrinmalesandfemales>40yrorwhoaremenopausal,orat
any age for adults with additional dyslipidemia risk factors (see sidebar)
• screenforsecondarycauses:hypothyroidism,chronickidneydisease,DM,nephroticsyndrome,liver
disease
• risk category
■ estimate using the Framingham Risk Score (FRS) for assessing 10 yr risk of developing CAD ◆ FRS is calculated based on gender, age, HDL-C, total cholesterol, sBP, smoking, DM
◆ family history of CVD <55 male relative or <65 in female relative doubles FRS
◆ to be completed for men and women age 40-75 q3-5yr
◆ cardiovascular age calculated as patient’s age ± the difference between his or her estimated remaining life expectancy
◆ used to increase adherence to therapy and reaffirm positive effect of following therapy
■ treatment decisions focus on LDL-C level and/or FRS risk; the alternate primary targets are
apolipoprotein B (apo B) and non-HDL-C
■ if moderate risk and LDL-C <3.5, treatment decision thresholds shifted to apo B >1.2 g/L or non-
HDL-C >4.3 mmol/L
■ other targets include: TC:HDL-C ratio, apo B:apo AI ratio, hs-CRP (used more for risk stratification
of CAD), non-HDL-C, and serum TG levels
