
Page 42 - TNFlipTest
P. 42
A8 Anesthesia
Airway Management
Toronto Notes 2019
Table 2. Methods of Supporting the Airway
Equipment for Intubation
MDSOLES
Monitors
Drugs
Suction
Oxygen source and self-inflating bag with oropharyngeal and nasopharyngeal airways Laryngoscope
Endotracheal tubes (appropriate size and one size smaller)
Stylet, Syringe for tube cuff inflation
Medications that can be Given Through the ETT
Advantages/ Indications
Disadvantages/ Contraindications
Other
Bag and Mask
Basic Non-invasive Readily available
Risk of aspiration if decreased LOC Cannot ensure airway patency
Inability to deliver precise tidal volume
Operator fatigue
Facilitate airway patency with jaw thrust and chin lift Can use oropharyngeal/ nasopaharyngeal airway
Laryngeal Mask Airway (LMA)
Easy to insert
Less airway trauma/irritation than ETT
Frees up hands (vs. face mask) Primarily used in spontaneously ventilating patient
Risk of gastric aspiration
PPV <20 cm H20 needed Oropharyngeal/retropharyngeal pathology or foreign body Does not protect against laryngospasm or gastric aspiration
Sizing by body weight (approx) 40-50 kg: 3
50-70 kg: 4
70-100 kg: 5
Endotracheal Tube (ETT)
Indications for intubation (5 Ps) Patent airway
Protects against aspiration Positive pressure ventilation Pulmonary toilet (suction) Pharmacologic administration during hemodynamic instability
Insertion can be difficult
Muscle relaxant usually needed Most invasive – see Complications During Laryngoscopy and Intubation, A9
Auscultate to avoid endobronchial intubation
Sizing (approx):
Male: 8.0-9.0 mm
Female: 7.0-8.0 mm Pediatric Uncuffed (>age 2): (age/4) + 4 mm
Tracheal Intubation
Preparing for Intubation
NAVEL Naloxone Atropine Ventolin Epinephrine Lidocaine
A.
Tongue Epiglottis
Trachea Esophagus
B.
C.
Oral axis (OA)
• failedattemptsatintubationcanmakefurtherattemptsmoredifficultduetotissuetrauma
• plan,prepare,andassessforpotentialdifficulties(seePre-OperativeAssessment,A2)
• ensureequipmentisavailableandworking(testETTcuff,checklaryngoscopelightandsuction,
machine check)
• pre-oxygenate/denitrogenate:patientbreathes100%O2for3-5minorfor4-8vitalcapacitybreaths • mayneedtosuctionmouthandpharynxfirst
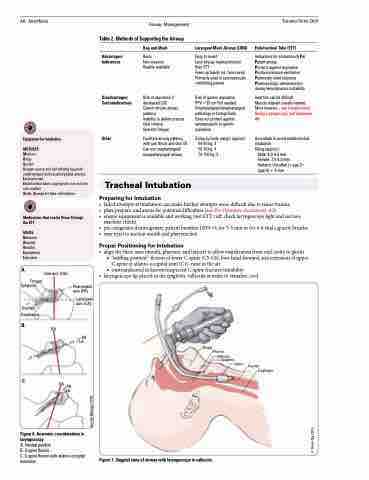
Proper Positioning for Intubation
• alignthethreeaxes(mouth,pharynx,andlarynx)toallowvisualizationfromoralcavitytoglottis
■ “sniffing position”: flexion of lower C-spine (C5-C6), bow head forward, and extension of upper
C-spine at atlanto-occipital joint (C1), nose in the air
■ contraindicated in known/suspected C-spine fracture/instability
• laryngoscopetipplacedintheepiglotticvalleculainordertovisualizecord
Tongue Pharynx
OA
Pharyngeal axis (PA)
Laryngeal axis (LA)
PA LA
OA PA LA
Figure 6. Anatomic considerations in laryngoscopy
A. Neutral position
B. C-spine flexion
C. C-spine flexion with atlanto-occipital extension
Figure 7. Saggital view of airway with laryngoscope in vallecula
Vallecula Epiglottis
Glottis Trachea Esophagus
© Derek Ng 2015
© Jennifer Belanger 2009
