
Page 435 - TNFlipTest
P. 435
Toronto Notes 2019
Colorectal Neoplasms
General Surgery and Thoracic Surgery GS33
Colorectal Neoplasms
Colorectal Polyps
Definition
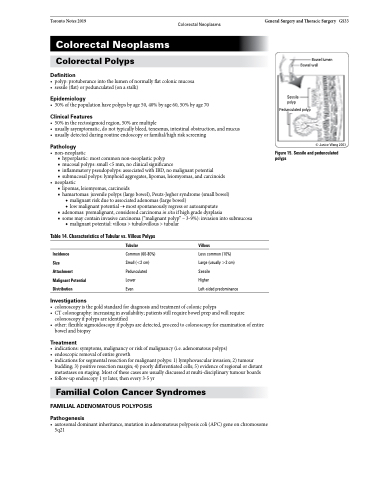
• polyp:protuberanceintothelumenofnormallyflatcolonicmucosa • sessile(flat)orpedunculated(onastalk)
Epidemiology
• 30%ofthepopulationhavepolypsbyage50,40%byage60,50%byage70
Clinical Features
• 50%intherectosigmoidregion,50%aremultiple
• usuallyasymptomatic,donottypicallybleed,tenesmus,intestinalobstruction,andmucus • usuallydetectedduringroutineendoscopyorfamilial/highriskscreening
Pathology
• non-neoplastic
■ hyperplastic: most common non-neoplastic polyp
■ mucosal polyps: small <5 mm, no clinical significance
■ inflammatory pseudopolyps: associated with IBD, no malignant potential
■ submucosal polyps: lymphoid aggregates, lipomas, leiomyomas, and carcinoids
• neoplastic
■ lipomas, leiomyomas, carcinoids
■ hamartomas: juvenile polyps (large bowel), Peutz-Jegher syndrome (small bowel)
◆ malignant risk due to associated adenomas (large bowel)
◆ low malignant potential → most spontaneously regress or autoamputate
■ adenomas: premalignant, considered carcinoma in situ if high grade dysplasia
■ some may contain invasive carcinoma (“malignant polyp” – 3-9%): invasion into submucosa
Bowel lumen Bowel wall
◆ malignant potential: villous > tubulovillous > tubular
Table 14. Characteristics of Tubular vs. Villous Polyps
Sessile polyp
Pedunculated polyp
Figure15.Sessileandpedunculated polyps
© Janice Wong 2003
Incidence
Size
Attachment Malignant Potential Distribution
Investigations
Tubular
Common (60-80%) Small (<2 cm) Pedunculated Lower
Even
Villous
Less common (10%) Large (usually >2 cm) Sessile
Higher
Left-sided predominance
• colonoscopyisthegoldstandardfordiagnosisandtreatmentofcolonicpolyps
• CTcolonography:increasinginavailability;patientsstillrequirebowelprepandwillrequire
colonoscopy if polyps are identified
• other:flexiblesigmoidoscopyifpolypsaredetected,proceedtocolonoscopyforexaminationofentire
bowel and biopsy
Treatment
• indications:symptoms,malignancyorriskofmalignancy(i.e.adenomatouspolyps)
• endoscopicremovalofentiregrowth
• indicationsforsegmentalresectionformalignantpolyps:1)lymphovascularinvasion;2)tumour
budding; 3) positive resection margin; 4) poorly differentiated cells; 5) evidence of regional or distant
metastases on staging. Most of these cases are usually discussed at multi-disciplinary tumour boards • follow-upendoscopy1yrlater,thenevery3-5yr
Familial Colon Cancer Syndromes
FAMILIAL ADENOMATOUS POLYPOSIS
Pathogenesis
• autosomaldominantinheritance,mutationinadenomatouspolyposiscoli(APC)geneonchromosome 5q21
