
Page 437 - TNFlipTest
P. 437
Toronto Notes 2019
Colorectal Neoplasms
General Surgery and Thoracic Surgery GS35 Removed
LAR
APR
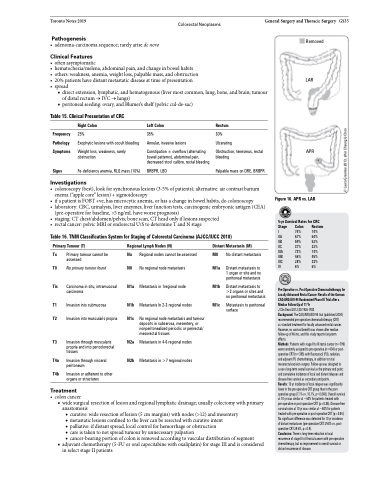
Figure 16. APR vs. LAR
5-yr Survival Rates for CRC Stage Colon Rectum I 74% 74%
IIA 67% 64%
IIB 59% 52%
IIC 37% 32% IIIA 73% 74% IIIB 46% 45% IIIC 28% 33%
IV 6% 6%
Pre-Operative vs. Post-Operative Chemoradiotherapy for Locally Advanced Rectal Cancer: Results of the German CAO/ARO/AIO-94 Randomized Phase III Trial after a Median Follow-Up of 11 Yr
J Clin Oncol 2012;30:1926-1933
Background: The CAO/ARO/AIO-94 trial (published 2004) recommended pre-operative chemoradiotherapy (CRT)
as standard treatment for locally advanced rectal cancer. However, no survival benefit was shown after median follow-up of 46 mo, and this study reports long-term effects.
Methods: Patients with stage II to III rectal cancer (n=799) were randomly assigned to pre-operative (n=404) or post- operative CRT (n=395) with fluorouracil (FU), radiation, and adjuvant FU chemotherapy, in addition to total mesorectal excision surgery. Follow-up was designed to assess long-term overall survival as the primary end point; and cumulative incidence of local and distant relapses and disease-free survival as secondary end points.
Results: 10 yr incidence of local relapse was significantly lower in the pre-operative CRT group than in the post- operative group (7.1% vs. 10.1%, p=0.048). Overall survival at 10 yr was similar at ~60% for patients treated with pre-operative or post-operative CRT (p=0.85). Disease-free survival rates at 10 yr was similar at ~68% for patients treated with pre-operative or post-operative CRT (p=0.54). No significant difference was detected for 10 yr incidence of distant metastases (pre-operative CRT 29.8% vs. post- operative CRT 29.6%, p=0.9).
Conclusion: There is long-term reduction in local recurrence of stage II to III rectal cancer with pre-operative chemotherapy, but no improvement in overall survival or distant recurrence of disease.
Pathogenesis
• adenoma-carcinomasequence;rarelyarisedenovo
Clinical Features
• oftenasymptomatic
• hematochezia/melena,abdominalpain,andchangeinbowelhabits
• others:weakness,anemia,weightloss,palpablemass,andobstruction • 20%patientshavedistantmetastaticdiseaseattimeofpresentation
• spread
■ direct extension, lymphatic, and hematogenous (liver most common, lung, bone, and brain; tumour of distal rectum → IVC → lungs)
■ peritoneal seeding: ovary, and Blumer’s shelf (pelvic cul-de-sac)
Table 15. Clinical Presentation of CRC
Frequency Pathology Symptoms
Signs
Right Colon
25%
Exophytic lesions with occult bleeding
Weight loss, weakness, rarely obstruction
Fe-deficiency anemia, RLQ mass (10%)
Left Colon
35%
Annular, invasive lesions
Constipation ± overflow (alternating bowel patterns), abdominal pain, decreased stool calibre, rectal bleeding
BRBPR, LBO
Rectum
30% Ulcerating
Obstruction, tenesmus, rectal bleeding
Palpable mass on DRE, BRBPR
Investigations
• colonoscopy(best),lookforsynchronouslesions(3-5%ofpatients);alternative:aircontrastbarium enema (“apple core” lesion) + sigmoidoscopy
• ifapatientisFOBT+ve,hasmicrocyticanemia,orhasachangeinbowelhabits,docolonoscopy
• laboratory:CBC,urinalysis,liverenzymes,liverfunctiontests,carcinogenicembryonicantigen(CEA)
(pre-operative for baseline, >5 ng/mL have worse prognosis)
• staging:CTchest/abdomen/pelvis;bonescan,CTheadonlyiflesionssuspected
• rectalcancer:pelvicMRIorendorectalU/StodetermineTandNstage
Table 16. TNM Classification System for Staging of Colorectal Carcinoma (AJCC/IUCC 2010)
Primary Tumour (T)
Tx Primary tumour cannot be assessed
T0 No primary tumour found
Tis Carcinoma in situ, intramucosal
carcinoma
T1 Invasion into submucosa
T2 Invasion into muscularis propria
T3 Invasion through muscularis propria and into pericolorectal
tissues
T4a Invasion through visceral peritoneum
T4b Invasion or adherent to other organs or structures
Treatment
Regional Lymph Nodes (N)
Nx Regional nodes cannot be assessed N0 No regional node metastasis
N1a Metastasis in 1regional node N1b Metastasis In 2-3 regional nodes
N1c No regional node metastasis and tumour deposits in subserosa, mesentery, or nonperitonealized pericolic or perirectal/ mesorectal tissues
N2a Metastasis in 4-6 regional nodes N2b Metastasis in >7 regional nodes
Distant Metastasis (M)
M0 No distant metastasis
M1a Distant metastasis to 1 organ or site and no peritoneal metastasis
M1b Distant metastasis to >2 organs or sites and
no peritoneal metastasis
M1c Metastasis to peritoneal surface
• coloncancer
■ wide surgical resection of lesion and regional lymphatic drainage; usually colectomy with primary
anastomosis
◆ curative: wide resection of lesion (5 cm margins) with nodes (>12) and mesentery
◆ metastatic lesions confined to the liver can be resected with curative intent
◆ palliative: if distant spread, local control for hemorrhage or obstruction
◆ care is taken to not spread tumour by unnecessary palpation
◆ cancer-bearing portion of colon is removed according to vascular distribution of segment
■ adjuvant chemotherapy (5-FU or oral capecitabine with oxaliplatin) for stage III and is considered in select stage II patients
© Laura Greenlee 2013, after Cheung & Chen
