
Page 504 - TNFlipTest
P. 504
GY18 Gynecology
Termination of Pregnancy
Toronto Notes 2019
Emergency Postcoital Contraception
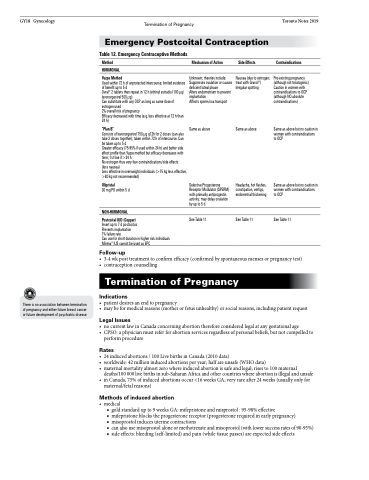
Table 12. Emergency Contraceptive Methods
Method
HORMONAL
Yuzpe Method
Used within 72 h of unprotected intercourse; limited evidence of benefit up to 5 d
Ovral® 2 tablets then repeat in 12 h (ethinyl estradiol 100 μg/ levonorgestrel 500 μg)
Can substitute with any OCP as long as same dose of estrogen used
2% overall risk of pregnancy
Efficacy decreased with time (e.g. less effective at 72 h than 24 h)
“Plan B”
Consists of levonorgestrel 750 μg q12h for 2 doses (can also take 2 doses together); taken within 72 h of intercourse. Can betakenupto5d
Greater efficacy (75-95% if used within 24 h) and better side effect profile than Yuzpe method but efficacy decreases with time; 1st line if >24 h
No estrogen thus very few contraindications/side effects
(less nausea)
Less effective in overweight individuals (>75 kg less effective, >80 kg not recommended)
Ulipristal
30mgPOwithin5d
NON-HORMONAL
Postcoital IUD (Copper)
Insert up to 7 d postcoitus
Prevents implantation
1% failure rate
Can use for short duration in higher risk individuals Mirena® IUS cannot be used as EPC
Follow-up
Mechanism of Action
Unknown; theories include: Suppresses ovulation or causes deficient luteal phase
Alters endometrium to prevent implantation
Affects sperm/ova transport
Same as above
Selective Progesterone Receptor Modulator (SPERM) with primarily antiprogestin activity: may delay ovulation byupto5d
See Table 11
Side Effects
Nausea (due to estrogen; treat with Gravol®) Irregular spotting
Same as above
Headache, hot flashes, constipation, vertigo, endometrial thickening
See Table 11
Contraindications
Pre-existing pregnancy (although not teratogenic) Caution in women with contraindications to OCP (although NO absolute contraindications)
Same as above but no caution in women with contraindications to OCP
Same as above but no caution in women with contraindications to OCP
See Table 11
There is no association between termination of pregnancy and either future breast cancer or future development of psychiatric disease
• 3-4wkposttreatmenttoconfirmefficacy(confirmedbyspontaneousmensesorpregnancytest) • contraceptioncounselling
Termination of Pregnancy
Indications
• patientdesiresanendtopregnancy
• maybeformedicalreasons(motherorfetusunhealthy)orsocialreasons,includingpatientrequest
Legal Issues
• nocurrentlawinCanadaconcerningabortionthereforeconsideredlegalatanygestationalage
• CPSO:aphysicianmustreferforabortionservicesregardlessofpersonalbeliefs,butnotcompelledto
perform procedure
Rates
• 24inducedabortions/100LivebirthsinCanada(2010data)
• worldwide:42millioninducedabortionsperyear;halfareunsafe(WHOdata)
• maternalmortalityalmostzerowhereinducedabortionissafeandlegal;risesto100maternal
deaths/100 000 live births in sub-Saharan Africa and other countries where abortion is illegal and unsafe • inCanada,75%ofinducedabortionsoccur<16weeksGA;veryrareafter24weeks(usuallyonlyfor
maternal/fetal reasons)
Methods of induced abortion
• medical
■ gold standard up to 9 weeks GA: mifepristone and misprostol : 95-98% effective
■ mifepristone blocks the progesterone receptor (progesterone required in early pregnancy)
■ misoprostol induces uterine contractions
■ canalsousemisoprostolaloneormethotrexateandmisoprostol(withlowersuccessratesof90-95%) ■ side effects: bleeding (self-limited) and pain (while tissue passes) are expected side effects
