
Page 55 - TNFlipTest
P. 55
Toronto Notes 2019
Regional Anesthesia
Anesthesia A21
Table 13. Epidural vs. Spinal Anesthesia
Deposition Site
Onset
Effectiveness Difficulty
Patient Positioning
Specific Gravity/ Spread
Dosage
Continuous Infusion
Complications
Combined Spinal- Epidural
Epidural
LA injected in epidural space (space between ligamentum flavum and dura)
Initial blockade is at the spinal roots followed by some degree of spinal cord anesthesia as LA diffuses into the subarachnoid space through the dura
Significant blockade requires 10-15 min Slower onset of side effects
Effectiveness of blockade can be variable Technically more difficult; greater failure rate
Position of patient not as important; specific gravity not an issue
Epidural injections spread throughout the potential space; specific gravity of solution does not affect spread
Larger volume/dose of LA (usually > toxic IV dose)
Use of catheter allows for continuous infusion or repeat injections
Failure of technique
Hypotension
Bradycardia if cardiac sympathetics blocked (only if ~T2-4 block), e.g. “high spinal”
Epidural or subarachnoid hematoma
Accidental subarachnoid injection can produce spinal anesthesia (and any of the above complications) Systemic toxicity of LA (accidental intravenous) Catheter complications (shearing, kinking, vascular or subarachnoid placement)
Infection
Dural puncture
Spinal
LA injected into subarachnoid space in the dural sac surrounding the spinal cord and nerve roots
Rapid blockade (onset in 2-5 min)
Very effective blockade
Easier to perform due to visual confirmation of CSF flow Hyperbaric LA solution – position of patient important
LA solution may be made hyperbaric (of greater specific gravity than the cerebrospinal fluid by mixing with 10% dextrose, thus increasing spread of LA to the dependent (low) areas of the subarachnoid space)
Smaller dose of LA required (usually < toxic IV dose) None
Failure of technique
Hypotension
Bradycardia if cardiac sympathetics blocked (only if ~T2-4 block), e.g. “high spinal”
Epidural or subarachnoid hematoma
Post-spinal headache (CSF leak)
Transient paresthesias
Spinal cord trauma, infection
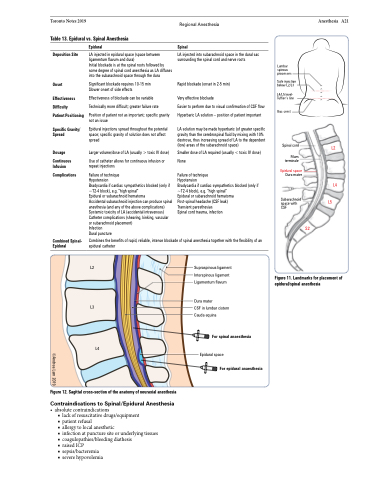
Lumbar spinous processes
Safe injection below L2/L3
L4/L5 level- Tuffier’s line
Iliac crest
Spinal cord
Filum terminale
Epidural space
Dura mater
Subarachnoid space with CSF
L2
L4
L5
Combines the benefits of rapid, reliable, intense blockade of spinal anesthesia together with the flexibility of an epidural catheter
S2
L2
Supraspinous ligament Interspinous ligament Ligamentum flavum
Dura mater
CSF in lumbar cistern Cauda equina
For spinal anaesthesia
Epidural space
For epidural anaesthesia
Figure 11. Landmarks for placement of epidural/spinal anesthesia
L4
Figure 12. Sagittal cross-section of the anatomy of neuraxial anesthesia
Contraindications to Spinal/Epidural Anesthesia
• absolutecontraindications
■ lack of resuscitative drugs/equipment
■ patient refusal
■ allergy to local anesthetic
■ infection at puncture site or underlying tissues ■ coagulopathies/bleeding diathesis
■ raised ICP
■ sepsis/bacteremia
■ severe hypovolemia
L3
©Andrea Lam 2019
