
Page 605 - TNFlipTest
P. 605
Toronto Notes 2019 Principles of Microbiology Mycology
Fungal Basics
• fungiareeukaryoticorganisms,theycanhavethefollowingmorphologies
1. yeast (unicellular)
2. moulds, also known as filamentous fungi (multicellular with hyphae)
3. dimorphic fungi (found as mould at room temperature but grow as yeast-like forms at body
Infectious Diseases ID5
Yeast
Mold: septate hyphae
Mold: non-septate hyphae Figure 4. Common fungus morphology
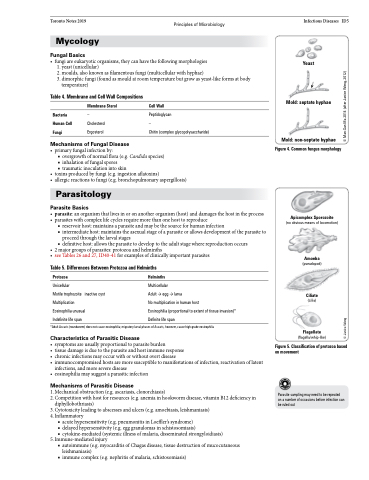
Apicomplex Sporozoite
(no obvious means of locomotion)
Amoeba
(pseudopod)
Ciliate
(cilia)
Flagellate
(flagella/whip-like)
Figure 5. Classification of protozoa based on movement
Parasite sampling may need to be repeated on a number of occasions before infection can be ruled out
temperature)
Table 4. Membrane and Cell Wall Compositions
Bacteria Human Cell Fungi
Membrane Sterol
– Cholesterol Ergosterol
Cell Wall
Peptidoglycan
–
Chitin (complex glycopolysaccharide)
Mechanisms of Fungal Disease
• primaryfungalinfectionby:
■ overgrowth of normal flora (e.g. Candida species) ■ inhalation of fungal spores
■ traumatic inoculation into skin
• toxinsproducedbyfungi(e.g.ingestionaflatoxins)
• allergicreactionstofungi(e.g.bronchopulmonaryaspergillosis)
Parasitology
Parasite Basics
• parasite:anorganismthatlivesinoronanotherorganism(host)anddamagesthehostintheprocess • parasiteswithcomplexlifecyclesrequiremorethanonehosttoreproduce
■ reservoir host: maintains a parasite and may be the source for human infection
■ intermediate host: maintains the asexual stage of a parasite or allows development of the parasite to
proceed through the larval stages
■ definitive host: allows the parasite to develop to the adult stage where reproduction occurs
• 2majorgroupsofparasites:protozoaandhelminths
• seeTables26and27,ID40-41forexamplesofclinicallyimportantparasites
Table 5. Differences Between Protozoa and Helminths
Protozoa
Unicellular
Motile trophozoite
Multiplication
Helminths
Multicellular
Adult → egg → larva
No multiplication in human host
Eosinophilia (proportional to extent of tissue invasion)* Definite life span
• symptomsareusuallyproportionaltoparasiteburden
• tissuedamageisduetotheparasiteandhostimmuneresponse
• chronicinfectionsmayoccurwithorwithoutovertdisease
• immunocompromisedhostsaremoresusceptibletomanifestationsofinfection,reactivationoflatent
infections, and more severe disease
• eosinophiliamaysuggestaparasiticinfection
Mechanisms of Parasitic Disease
1. Mechanical obstruction (e.g. ascariasis, clonorchiasis)
2. Competition with host for resources (e.g. anemia in hookworm disease, vitamin B12 deficiency in
diphyllobothriasis)
3. Cytotoxicity leading to abscesses and ulcers (e.g. amoebiasis, leishmaniasis)
4. Inflammatory
■ acute hypersensitivity (e.g. pneumonitis in Loeffler’s syndrome)
■ delayed hypersensitivity (e.g. egg granulomas in schistosomiasis)
■ cytokine-mediated (systemic illness of malaria, disseminated strongyloidiasis)
5. Immune-mediated injury
■ autoimmune (e.g. myocarditis of Chagas disease, tissue destruction of mucocutaneous
leishmaniasis)
■ immune complex (e.g. nephritis of malaria, schistosomiasis)
Eosinophilia unusual
inactive cyst
Indefinite life span
*Adult Ascaris (roundworm) does not cause eosinophilia; migratory larval phases of Ascaris, however, cause high-grade eosinophilia
Characteristics of Parasitic Disease
© Janice Wong © Man-San Ma 2014 (after Janice Wong, 2012)
