
Page 664 - TNFlipTest
P. 664
MG6 Medical Genetics Syndromes and Diseases
Toronto Notes 2019
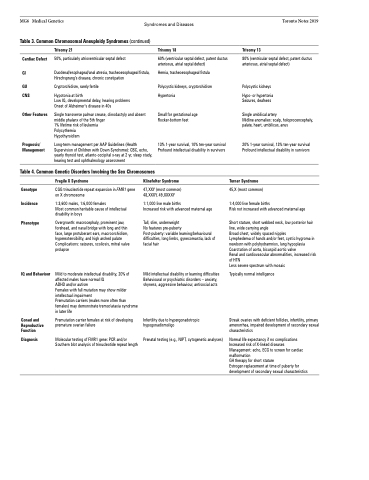
Table 3. Common Chromosomal Aneuploidy Syndromes (continued)
Cardiac Defect
GI
GU CNS
Other Features
Prognosis/ Management
Trisomy 21
50%, particularly atrioventricular septal defect
Duodenal/esophageal/anal atresia, tracheoesophageal fistula, Hirschsprung’s disease, chronic constipation
Cryptorchidism, rarely fertile
Hypotonia at birth
Low IQ, developmental delay, hearing problems Onset of Alzheimer’s disease in 40s
Single transverse palmar crease, clinodactyly and absent middle phalanx of the 5th finger
1% lifetime risk of leukemia
Polycythemia
Hypothyroidism
Long-term management per AAP Guidelines (Health Supervision of Children with Down Syndrome): CBC, echo, yearly thyroid test, atlanto-occipital x-ray at 2 yr, sleep study, hearing test and ophthalmology assessment
Trisomy 18
60% (ventricular septal defect, patent ductus arteriosus, atrial septal defect)
Hernia, tracheoesophageal fistula
Polycystic kidneys, cryptorchidism Hypertonia
Small for gestational age Rocker-bottom feet
13% 1-year survival, 10% ten-year survival Profound intellectual disability in survivors
Trisomy 13
80% (ventricular septal defect, patent ductus arteriosus, atrial septal defect)
Polycystic kidneys
Hypo- or hypertonia Seizures, deafness
Single umbilical artery
Midline anomalies: scalp, holoprocencephaly, palate, heart, umbilicus, anus
20% 1-year survival, 13% ten-year survival Profound intellectual disability in survivors
Turner Syndrome
45,X (most common)
1:4,000 live female births
Risk not increased with advanced maternal age
Short stature, short webbed neck, low posterior hair line, wide carrying angle
Broad chest, widely spaced nipples
Lymphedema of hands and/or feet, cystic hygroma in newborn with polyhydramnios, lung hypoplasia Coarctation of aorta, bicuspid aortic valve
Renal and cardiovascular abnormalities, increased risk of HTN
Less severe spectrum with mosaic
Typically normal intelligence
Streak ovaries with deficient follicles, infertility, primary amenorrhea, impaired development of secondary sexual characteristics
Normal life expectancy if no complications Increased risk of X-linked diseases Management: echo, ECG to screen for cardiac malformation
GH therapy for short stature
Estrogen replacement at time of puberty for development of secondary sexual characteristics
Table 4. Common Genetic Disorders Involving the Sex Chromosomes
Genotype Incidence
Phenotype
IQ and Behaviour
Gonad and Reproductive Function
Diagnosis
Fragile X Syndrome
CGG trinucleotide repeat expansion in FMR1 gene on X chromosome
1:3,600 males, 1:6,000 females
Most common heritable cause of intellectual disability in boys
Overgrowth: macrocephaly, prominent jaw, forehead, and nasal bridge with long and thin face, large protuberant ears, macroorchidism, hyperextensibility, and high arched palate Complications: seizures, scoliosis, mitral valve prolapse
Mild to moderate intellectual disability, 20% of affected males have normal IQ
ADHD and/or autism
Females with full mutation may show milder intellectual impairment
Premutation carriers (males more often than females) may demonstrate tremor/ataxia syndrome in later life
Premutation carrier females at risk of developing premature ovarian failure
Molecular testing of FMR1 gene: PCR and/or Southern blot analysis of trinucleotide repeat length
Klinefelter Syndrome
47,XXY (most common) 48,XXXY, 49,XXXXY
1:1,000 live male births
Increased risk with advanced maternal age
Tall, slim, underweight
No features pre-puberty
Post-puberty: variable learning/behavioural difficulties, long limbs, gynecomastia, lack of facial hair
Mild intellectual disability or learning difficulties Behavioural or psychiatric disorders – anxiety, shyness, aggressive behaviour, antisocial acts
Infertility due to hypergonadotropic hypogonadismoligo
Prenatal testing (e.g., NIPT, cytogenetic analyses)
