
Page 677 - TNFlipTest
P. 677
Toronto Notes 2019 Chest Imaging
Pneumothorax
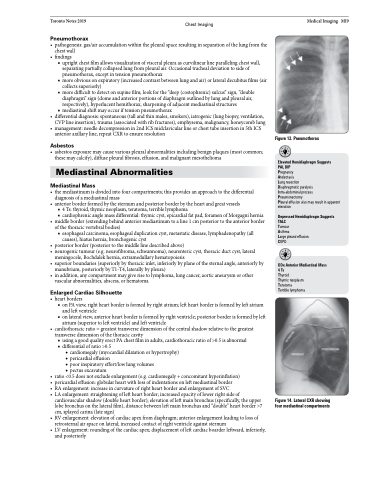
• pathogenesis:gas/airaccumulationwithinthepleuralspaceresultinginseparationofthelungfromthe chest wall
• findings
■ upright chest film allows visualization of visceral pleura as curvilinear line paralleling chest wall,
separating partially collapsed lung from pleural air. Occasional tracheal deviation to side of
pneumothorax, except in tension pneumothorax
■ more obvious on expiratory (increased contrast between lung and air) or lateral decubitus films (air
collects superiorly)
■ more difficult to detect on supine film; look for the “deep (costophrenic) sulcus” sign, “double
diaphragm” sign (dome and anterior portions of diaphragm outlined by lung and pleural air,
respectively), hyperlucent hemithorax, sharpening of adjacent mediastinal structures ■ mediastinal shift may occur if tension pneumothorax
• differentialdiagnosis:spontaneous(tallandthinmales,smokers),iatrogenic(lungbiopsy,ventilation, CVP line insertion), trauma (associated with rib fractures), emphysema, malignancy, honeycomb lung
• management:needledecompressionin2ndICSmidclavicularlineorchesttubeinsertionin5thICS anterior axillary line, repeat CXR to ensure resolution
Asbestos
• asbestosexposuremaycausevariouspleuralabnormalitiesincludingbenignplaques(mostcommon; these may calcify), diffuse pleural fibrosis, effusion, and malignant mesothelioma
Mediastinal Abnormalities
Mediastinal Mass
• themediastinumisdividedintofourcompartments;thisprovidesanapproachtothedifferential diagnosis of a mediastinal mass
• anteriorborderformedbythesternumandposteriorborderbytheheartandgreatvessels
■ 4 Ts: thyroid, thymic neoplasm, teratoma, terrible lymphoma
■ cardiophrenic angle mass differential: thymic cyst, epicardial fat pad, foramen of Morgagni hernia
• middle border (extending behind anterior mediastinum to a line 1 cm posterior to the anterior border of the thoracic vertebral bodies)
■ esophageal carcinoma, esophageal duplication cyst, metastatic disease, lymphadenopathy (all causes), hiatus hernia, bronchogenic cyst
• posteriorborder(posteriortothemiddlelinedescribedabove)
• neurogenictumour(e.g.neurofibroma,schwannoma),neurentericcyst,thoracicductcyst,lateral
meningocele, Bochdalek hernia, extramedullary hematopoiesis
• superiorboundaries(superiorlybythoracicinlet,inferiorlybyplaneofthesternalangle,anteriorlyby
manubrium, posteriorly by T1-T4, laterally by pleura)
• in addition, any compartment may give rise to lymphoma, lung cancer, aortic aneurysm or other
vascular abnormalities, abscess, or hematoma
Enlarged Cardiac Silhouette
• heartborders
■ on PA view, right heart border is formed by right atrium; left heart border is formed by left atrium
and left ventricle
■ on lateral view, anterior heart border is formed by right ventricle; posterior border is formed by left
atrium (superior to left ventricle) and left ventricle
• cardiothoracicratio=greatesttransversedimensionofthecentralshadowrelativetothegreatest
transverse dimension of the thoracic cavity
■ using a good quality erect PA chest film in adults, cardiothoracic ratio of >0.5 is abnormal ■ differential of ratio >0.5
◆ cardiomegaly (myocardial dilatation or hypertrophy) ◆ pericardial effusion
◆ poor inspiratory effort/low lung volumes
◆ pectus excavatum
• ratio<0.5doesnotexcludeenlargement(e.g.cardiomegaly+concomitanthyperinflation)
• pericardialeffusion:globularheartwithlossofindentationsonleftmediastinalborder
• RAenlargement:increaseincurvatureofrightheartborderandenlargementofSVC
• LAenlargement:straighteningofleftheartborder;increasedopacityoflowerrightsideof
cardiovascular shadow (double heart border); elevation of left main bronchus (specifically, the upper lobe bronchus on the lateral film), distance between left main bronchus and “double” heart border >7 cm, splayed carina (late sign)
• RVenlargement:elevationofcardiacapexfromdiaphragm;anteriorenlargementleadingtolossof retrosternal air space on lateral; increased contact of right ventricle against sternum
• LVenlargement:roundingofthecardiacapex;displacementofleftcardiacboarderleftward,inferiorly, and posteriorly
Medical Imaging MI9
Figure 13. Pneumothorax
Elevated Hemidiaphragm Suggests PAL DIP
Pregnancy
Atelectasis
Lung resection
Diaphragmatic paralysis
Intra-abdominal process
Pneumonectomy
Pleural effusion also may result in apparent elevation
Depressed Hemidiaphragm Suggests TALC
Tumour
Asthma
Large pleural effusion COPD
DDx Anterior Mediastinal Mass 4Ts
Thyroid
Thymic neoplasm
Teratoma
Terrible lymphoma
Figure 14. Lateral CXR showing four mediastinal compartments
