
Page 710 - TNFlipTest
P. 710
NP10 Nephrology
Electrolyte Disorders Toronto Notes 2019
SYNDROME OF INAPPROPRIATE ANTIDIURETIC HORMONE SECRETION
1. urine that is inappropriately concentrated for the serum osmolality 2. high urine sodium (>20-40 mmol/L)
3. high FENa
Table 5. Disorders Associated with SIADH
Cancer
Small cell cancer Bronchogenic carcinoma Pancreatic adenocarcinoma Hodgkin’s lymphoma Thymoma
Leukemia
Pulmonary
Pneumonia
Lung abscess Tuberculosis
Acute respiratory failure Asthma
COPD
Positive pressure ventilation
CNS
Mass lesion Encephalitis Subarachnoid hemorrhage Stroke
Head trauma Acute psychosis Acute intermittent porphyria
Drugs
Antidepressants TCAs
SSRIs Antineoplastics Vincristine Cyclophosphamide Anti-epileptics Carbamazepine Barbiturates Chlorpropamide ACEI
Other DDAVP Oxytocin Nicotine
Miscellaneous
Post-operative state Pain
Severe nausea
HIV
Hypernatremia
• hypernatremia:serum[Na+]>145mmol/L
• toolittlewaterrelativetototalbodyNa+;alwaysahyperosmolarstate
• usually due to NET water loss, rarely due to hypertonic Na+ gain
• lesscommonthanhyponatremiabecausepatientsareprotectedagainsthypernatremiabythirstand
release of ADH
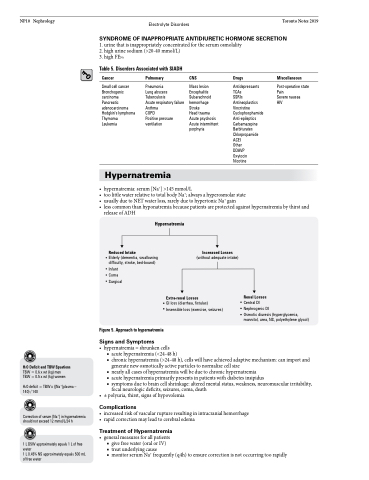
Reduced Intake
Elderly (dementia, swallowing difficulty, stroke, bed-bound)
Infant Coma Surgical
Figure 5. Approach to hypernatremia
Signs and Symptoms
Hypernatremia
Increased Losses
(without adequate intake)
Extra-renal Losses
GI loss (diarrhea, fistulas) Insensible loss (exercise, seizures)
Renal Losses
Central DI Nephrogenic DI
Osmotic diuresis (hyperglycemia, mannitol, urea, NS, polyethylene glycol)
H2O Deficit and TBW Equations
TBW=0.6xwt(kg)men TBW = 0.5 x wt (kg) women
H2O deficit = TBW x ([Na+]plasma – 140) / 140
Correction of serum [Na+] in hypernatremia should not exceed 12 mmol/L/24 h
1 L D5W approximately equals 1 L of free water
1 L 0.45% NS approximately equals 500 mL of free water
• hypernatremia=shrunkencells
■ acute hypernatremia (<24-48 h)
■ chronic hypernatremia (>24-48 h), cells will have achieved adaptive mechanism: can import and
generate new osmotically active particles to normalize cell size
■ nearly all cases of hypernatremia will be due to chronic hypernatremia
■ acute hypernatremia primarily presents in patients with diabetes insipidus
■ symptoms due to brain cell shrinkage: altered mental status, weakness, neuromuscular irritability,
focal neurologic deficits, seizures, coma, death • ±polyuria,thirst,signsofhypovolemia
Complications
• increasedriskofvascularruptureresultinginintracranialhemorrhage • rapidcorrectionmayleadtocerebraledema
Treatment of Hypernatremia
• generalmeasuresforallpatients
■ give free water (oral or IV)
■ treat underlying cause
■ monitor serum Na+ frequently (q4h) to ensure correction is not occurring too rapidly
