
Page 723 - TNFlipTest
P. 723
Toronto Notes 2019
Parenchymal Kidney Diseases
Nephrology NP23
3 . NEPHROTIC SYNDROME
Clinical/Lab Features
• heavyproteinuria(>3.5g/1.73m2/d)
• hypoalbuminemia
• edema
• hyperlipidemia(elevatedLDLcholesterol),lipiduria(fattycastsandovalfatbodieson
microscopy)
• hypercoagulablestate(duetoantithrombinIII,ProteinC,andProteinSurinarylosses)
• patientmayreportfrothyurine
• glomerularpathologyonrenalbiopsy(nephroticsyndromeisalwayscausedbyglomerularpathology,
unlike nephritic syndrome which may result from any parenchymal kidney disease)
■ minimal change disease (or minimal lesion disease or nil disease) – e.g. glomeruli appear normal on
light microscopy
■ membranous glomerulopathy
■ focal segmental glomerulosclerosis (FSGS)
■ membranoproliferative GN ■ nodular glomerulosclerosis
• eachcanbeidiopathicorsecondarytoasystemicdiseaseordrug(sirolimuscancauseproteinuria without obvious glomerular pathology)
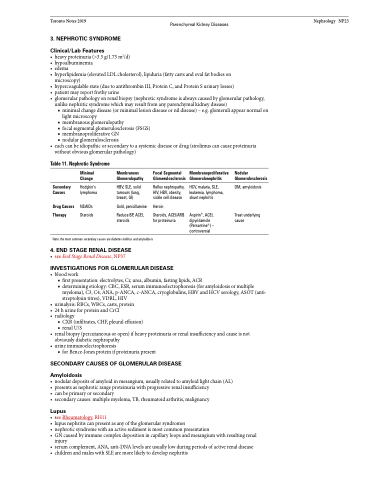
Table 11. Nephrotic Syndrome
Minimal Change
Hodgkin’s lymphoma
NSAIDs Steroids
Membranous Glomerulopathy
HBV, SLE, solid tumours (lung, breast, GI)
Gold, penicillamine
Reduce BP, ACEI, steroids
Focal Segmental Membranoproliferative Glomerulosclerosis Glomerulonephritis
Nodular Glomerulosclerosis
DM, amyloidosis
Treat underlying cause
Secondary Causes
Drug Causes Therapy
Reflux nephropathy, HIV, HBV, obesity, sickle cell disease
Heroin
Steroids, ACEI/ARB for proteinuria
HCV, malaria, SLE, leukemia, lymphoma, shunt nephritis
Aspirin®, ACEI, dipyridamole (Persantine®) – controversial
Note: the most common secondary causes are diabetes mellitus and amyloidosis
4 . END STAGE RENAL DISEASE
• seeEndStageRenalDisease,NP37
INVESTIGATIONS FOR GLOMERULAR DISEASE
• bloodwork
■ first presentation: electrolytes, Cr, urea, albumin, fasting lipids, ACR
■ determining etiology: CBC, ESR, serum immunoelectrophoresis (for amyloidosis or multiple
myeloma), C3, C4, ANA, p-ANCA, c-ANCA, cryoglobulins, HBV and HCV serology, ASOT (anti-
streptolysin titres), VDRL, HIV
• urinalysis: RBCs, WBCs, casts, protein
• 24hurineforproteinandCrCl
• radiology
■ CXR (infiltrates, CHF, pleural effusion)
■ renal U/S
• renalbiopsy(percutaneousoropen)ifheavyproteinuriaorrenalinsufficiencyandcauseisnot
obviously diabetic nephropathy
• urineimmunoelectrophoresis
■ for Bence-Jones protein if proteinuria present
SECONDARY CAUSES OF GLOMERULAR DISEASE
Amyloidosis
• nodulardepositsofamyloidinmesangium,usuallyrelatedtoamyloidlightchain(AL) • presentsasnephroticrangeproteinuriawithprogressiverenalinsufficiency
• canbeprimaryorsecondary
• secondarycauses:multiplemyeloma,TB,rheumatoidarthritis,malignancy
Lupus
• seeRheumatology,RH11
• lupusnephritiscanpresentasanyoftheglomerularsyndromes
• nephroticsyndromewithanactivesedimentismostcommonpresentation
• GNcausedbyimmunecomplexdepositionincapillaryloopsandmesangiumwithresultingrenal
injury
• serumcomplement,ANA,anti-DNAlevelsareusuallylowduringperiodsofactiverenaldisease • childrenandmaleswithSLEaremorelikelytodevelopnephritis
