
Page 755 - TNFlipTest
P. 755
Toronto Notes 2019
Cranial Nerve Deficits
Neurology N13
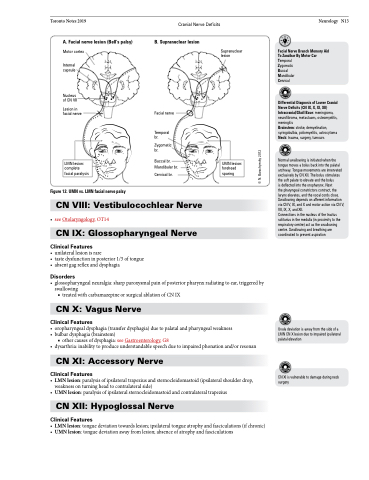
A. Facial nerve lesion (Bell’s palsy)
Motor cortex
Internal capsule
Nucleus of CN VII
Lesion in facial nerve
B. Supranuclear lesion
Facial nerve
Temporal br.
Zygomatic br.
Buccal br. Mandibular br. Cervical br.
Supranuclear lesion
Facial Nerve Branch Memory Aid To Zanzibar By Motor Car Temporal
Zygomatic
Buccal Mandibular Cervical
Differential Diagnosis of Lower Cranial Nerve Deficits (CN IX, X, XI, XII) Intracranial/Skull Base: meningioma, neurofibroma, metastases, osteomyelitis, meningitis
Brainstem: stroke, demyelination, syringobulbia, poliomyelitis, astrocytoma Neck: trauma, surgery, tumours
Normal swallowing is initiated when the tongue moves a bolus back into the palatal archway. Tongue movements are innervated exclusively by CN XII. The bolus stimulates the soft palate to elevate and the bolus
is deflected into the oropharynx. Next
the pharyngeal constrictors contract, the larynx elevates, and the vocal cords close. Swallowing depends on afferent information via CN V, IX, and X and motor action via CN V, VII, IX, X, and XII.
Connections in the nucleus of the tractus solitarius in the medulla (in proximity to the respiratory centre) act as the swallowing centre. Swallowing and breathing are coordinated to prevent aspiration
LMN lesion: complete facial paralysis
UMN lesion: forehead sparing
Figure 12. UMN vs. LMN facial nerve palsy
CN VIII: Vestibulocochlear Nerve
• seeOtolaryngology,OT14
CN IX: Glossopharyngeal Nerve
Clinical Features
• unilaterallesionisrare
• tastedysfunctioninposterior1/3oftongue • absentgagreflexanddysphagia
Disorders
• glossopharyngealneuralgia:sharpparoxysmalpainofposteriorpharynxradiatingtoear,triggeredby swallowing
■ treated with carbamazepine or surgical ablation of CN IX
CN X: Vagus Nerve
Clinical Features
• oropharyngealdysphagia(transferdysphagia)duetopalatalandpharyngealweakness • bulbardysphagia(brainstem)
■ other causes of dysphagia: see Gastroenterology, G8
• dysarthria:inabilitytoproduceunderstandablespeechduetoimpairedphonationand/orresonan
CN XI: Accessory Nerve
Clinical Features
• LMNlesion:paralysisofipsilateraltrapeziusandsternocleidomastoid(ipsilateralshoulderdrop, weakness on turning head to contralateral side)
• UMNlesion:paralysisofipsilateralsternocleidomastoidandcontralateraltrapezius CN XII: Hypoglossal Nerve
Clinical Features
• LMNlesion:tonguedeviationtowardslesion;ipsilateraltongueatrophyandfasciculations(ifchronic) • UMNlesion:tonguedeviationawayfromlesion;absenceofatrophyandfasciculations
Uvula deviation is away from the side of a LMN CN X lesion due to impaired ipsilateral palatal elevation
CN XI is vulnerable to damage during neck surgery
© N. Burachynsky 2012
