
Page 757 - TNFlipTest
P. 757
Toronto Notes 2019 Abnormalities of Visual Field Abnormalities of Visual Field
Neurology N15
Bitemporal Hemianopsia DDx by Age
• Children: craniopharyngioma
• Middle aged (20s to 50s): pituitary mass • Elderly (>60 yr): meningioma
In homonymous hemianopsia, more congruent deficits are caused by more posterior lesions; macular sparing may occur with occipital lesions
A lesion in a cerebral hemisphere causes eyes to “look away” from the hemiplegia, and to look towards the lesion
A lesion in the brainstem causes the eyes to “look toward” the side of the hemiplegia, and to look away from the lesion
Check all hemiplegic patients for homonymous hemianopsia (ipsilateral to side of hemiplegia)
Optic nerve 3 Optic chiasm
Optic tract
4
1 2
1 2 3
5 4 6
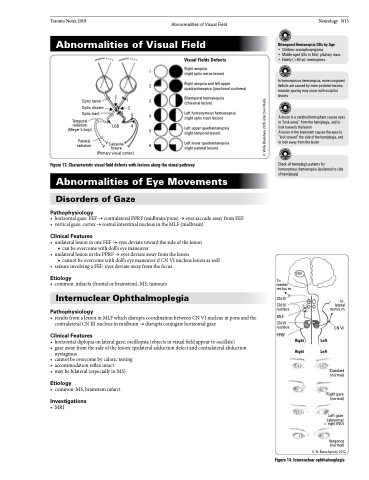
Visual Fields Defects
Right anopsia
(right optic nerve lesion)
Right anopsia and left upper quadrantanopsia (junctional scotoma)
Bitemporal hemianopsia (chiasmal lesion)
Left homonymous hemianopsia (right optic tract lesion)
Temporal
radiation (Meyer’s loop)
Parietal radiation
LGB
Left upper quadrantanopsia
5 (right temporal lesion)
Left lower quadrantanopsia
6 (right parietal lesion)
Calcarine fissure (Primary visual cortex)
Figure 13. Characteristic visual field defects with lesions along the visual pathway
Abnormalities of Eye Movements
Disorders of Gaze
Pathophysiology
• horizontalgaze:FEF→contralateralPPRF(midbrain/pons)→eyessaccadeawayfromFEF • verticalgaze:cortex→rostralinterstitialnucleusintheMLF(midbrain)
Clinical Features
• unilaterallesioninoneFEF→eyesdeviatetowardthesideofthelesion ■ can be overcome with doll’s eye maneuver
• unilaterallesioninthePPRF→eyesdeviateawayfromthelesion
■ cannot be overcome with doll’s eye maneuver if CN VI nucleus lesion as well
• seizureinvolvingaFEF:eyesdeviateawayfromthefocus
Etiology
• common:infarcts(frontalorbrainstem),MS,tumours
Internuclear Ophthalmoplegia
Pathophysiology
• resultsfromalesioninMLFwhichdisruptscoordinationbetweenCNVInucleusinponsandthe contralateral CN III nucleus in midbrain → disrupts conjugate horizontal gaze
Clinical Features
• horizontaldiplopiaonlateralgaze,oscillopsia(objectsinvisualfieldappeartooscillate)
• gazeawayfromthesideofthelesion:ipsilateraladductiondefectandcontralateralabduction
nystagmus
• cannotbeovercomebycalorictesting
• accommodationreflexintact
• maybebilateral(especiallyinMS)
Etiology
• common:MS,brainsteminfarct
Investigations
• MRI
FEF
CN III
CN III nucleus
MLF
CN VI nucleus
PPRF
To medial rectus m.
Right Right
Left Left
to lateral rectus m.
CN VI
Standard (normal)
Right gaze (normal)
Left gaze (abnormal = right INO)
Vergence (normal)
Figure 14. Internuclear ophthalmoplegia
© N. Burachynsky 2012
© Willa Bradshaw 2005 after Cecil Hahn
