
Page 763 - TNFlipTest
P. 763
Toronto Notes 2019 Behavioural Neurology
Mild Neurocognitive Disorder (Mild Cognitive Impairment)
Definition
• cognitiveimpairmentnotmeetingcriteriaofMajorNeurocognitiveDisorder
• measurabledeficitinatleastonecognitivedomainreportedbypatientorotherswithoutimpairmentin
ADLs
• amnestic(precursortoAD)vs.non-amnestic
Epidemiology
• mild NCD: 2-10% at age 65 yr and 5-25% by age 85 yr
Risk Factors
• vascular:hypertension,diabetesmellitus,obesity,cardiacdisease,apolipoproteinEepsilon4genotype
Clinical Features
• cognitiveimpairment
■ particularly in amnestic subtype
■ important to ascertain that memory complaints represent change from baseline
■ patients with mild NCD are often troubled by memory symptoms in comparison to patients with
dementia
• neuropsychiatricsymptoms
depression (50%), irritability, anxiety, aggression, and apathy
Investigations
• establishabaselineforfollow-up
• clinicalinterviewwithpatientandcaregiversisthecornerstoneofmildNCDevaluation • neuropsychologicaltesting
■ MMSE or MoCA; should not be used in isolation
■ if abnormal, follow-up in one year to monitor cognitive and functional decline • neuroimaging
■ role uncertain
■ most advocate for a non-contrast brain CT to evaluate for structural abnormalities (CVD, SDH,
NPH, or mass lesion) • othertesting
■ exclude treatable conditions and underlying psychiatric conditions
Treatment
• watchandwait
• noevidenceforcholinesteraseinhibitors,anti-inflammatoryagents,vascularriskfactormodification,
exercise, cognitive interventions
Prognosis
• 10%progresstomajorNCDperyr
• typicallyprogresstomajorNCDoveraperiodof2-3yr
Major Neurocognitive Disorder (formerly Dementia)
• seePsychiatry,PS12andGeriatricMedicine,GM4 Definition
• anacquired,generalized,and(usually)progressiveimpairmentofcognitivefunctionassociatedwith impairment in ADLs/iADLs (i.e. shopping, food preparation, finances, medication management)
• diagnosisofmajorNCDrequirespresenceofsignificantcognitivedeclinefromapreviouslevelof performance in one or more cognitive domains (complex attention, executive function, learning and memory, language, perceptual-motor, or social cognition) based on:
A) concern of the individual or a knowledgeable informant AND
B) a substantial impairment in cognitive performance either documented by standardized neuropsychological testing, or quantified clinical assessment
• seePsychiatry,PS28forDSM-5diagnosticcriteria
• incomparison,mildNCDdoesnotaffectADLs
■ mild NCD represents an intermediate stage between major NCD and normal aging
Epidemiology
• majorNCD:1-2%atage65yrandreachingashighas30%byage85yr • note
■ major NCD due to Alzheimer’s disease is uncommon before age 60 yr
■ major NCD due to frontotemporal lobar degeneration has an earlier onset and represents a
progressively smaller fraction of all NCDs with increasing age
Neurology N21
Delirium is a medical emergency carrying significant risk of morbidity and mortality; it is characterized by acute onset, disorientation, fluctuating level of consciousness, poor attention, and marked psychomotor changes
Visual hallucinations more commonly indicate organic disease
Prevalence of Depression in Patients with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis
JAMA Psychiatry 2017;74(1):58-67
Objectives: To estimate the prevalence of depression in individuals with mild cognitive impairment.
Methods: Review of articles with patients with mild cognitive impairment as a primary study group, reported depression/depressive symptoms using validated tool, and reported the prevalence of depression in patients with mild cognitive impairment.
Results: Pooled prevalence of depression patients with mild cognitive impairment was 32% (95% CI27-37%). Prevalenceincommunity-based populations (25%, 95% CI 19-30) was significantly lower than clinic-based populations (40%, 95%
CI 32-48).
Conclusions: Prevalence of depression in patients with mild cognitive impairment is high.
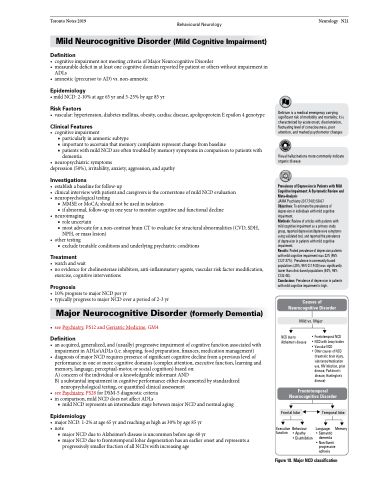
Causes of Neurocognitive Disorder
Mild vs. Major
NCD due to Alzheimer's disease
• Frontotemporal NCD • NCD with Lewy bodies • Vascular NCD
• Other causes of NCD
(traumatic brain injury, substance/medication use, HIV infection, prion disease, Parkinson's disease, Huntington's disease)
Frontotemporal Neurocognitive Disorder
Frontal lobe
Executive Behaviour:
Temporal lobe
Language: Memory • Semantic
dementia • Non-fluent
progressive aphasia
function
• Apathy
• Disinhibition
Figure 18. Major NCD classification
