
Page 86 - TNFlipTest
P. 86
C18 Cardiology and Cardiac Surgery
Arrhythmias
Toronto Notes 2019
Bradyarrhythmias
Bradyarrhythmias
• Examples
1. SA NODAL DYSFUNCTION
A. Sinus Bradycardia
P axis normal (P waves positive in I and aVF)
Rate <60 bpm ; marked sinus bradycardia (<50 bpm)
May be seen in normal adults, particularly athletes, and in elderly individuals
Increased vagal tone or vagal stimulation; drugs (β-blockers, calcium channel blockers, etc.); ischemia/infarction
2. AV CONDUCTION BLOCKS
A. First Degree AV Block
Prolonged PR interval (>200 msec)
Frequently found among otherwise healthy adults
B. Second Degree AV Block: Type I (Mobitz I)
A gradual prolongation of the PR interval precedes the failure of conduction of a P wave (Wenckebach phenomenon)
AV block is usually in AV node (proximal) triggers (usually reversible): increased vagal tone (e.g. following surgery), RCA-mediated ischemia
B. Second Degree AV Block: Type II (Mobitz II)
The PR interval is constant; there is an abrupt failure of conduction of a P wave
AV block is usually distal to the AV node (i.e. bundle of His); increased risk of high grade or 3rd degree AV block
B. Third Degree AV Block
Complete failure of conduction of the supraventricular impulses to the ventricles; ventricular depolarization initiated by an escape pacemaker distal to the block
Wide or narrow QRS, P-P and R-R intervals are constant, variable PR intervals; no relationship between P waves and QRS complexes (P waves “marching through”)
Atropine; pacing for sick sinus syndrome
No treatment required
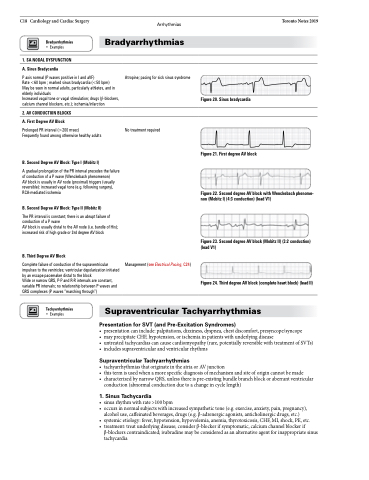
Figure 20. Sinus bradycardia
Figure 21. First degree AV block
Figure 22. Second degree AV block with Wenckebach phenome- non (Mobitz I) (4:3 conduction) (lead V1)
Figure 23. Second degree AV block (Mobitz II) (3:2 conduction) (lead V1)
Figure 24. Third degree AV block (complete heart block) (lead II)
Management (see Electrical Pacing, C24)
Tachyarrhythmias
• Examples
Supraventricular Tachyarrhythmias
Presentation for SVT (and Pre-Excitation Syndromes)
• presentationcaninclude:palpitations,dizziness,dyspnea,chestdiscomfort,presyncope/syncope
• mayprecipitateCHF,hypotension,orischemiainpatientswithunderlyingdisease
• untreatedtachycardiascancausecardiomyopathy(rare,potentiallyreversiblewithtreatmentofSVTs) • includessupraventricularandventricularrhythms
Supraventricular Tachyarrhythmias
• tachyarrhythmiasthatoriginateintheatriaorAVjunction
• thistermisusedwhenamorespecificdiagnosisofmechanismandsiteoforigincannotbemade
• characterizedbynarrowQRS,unlessthereispre-existingbundlebranchblockoraberrantventricular
conduction (abnormal conduction due to a change in cycle length)
1 . Sinus Tachycardia
• sinusrhythmwithrate>100bpm
• occursinnormalsubjectswithincreasedsympathetictone(e.g.exercise,anxiety,pain,pregnancy),
alcohol use, caffeinated beverages, drugs (e.g. β-adrenergic agonists, anticholinergic drugs, etc.)
• systemicetiology:fever,hypotension,hypovolemia,anemia,thyrotoxicosis,CHF,MI,shock,PE,etc.
• treatment:treatunderlyingdisease;considerβ-blockerifsymptomatic,calciumchannelblockerif
β-blockers contraindicated; ivabradine may be considered as an alternative agent for inappropriate sinus tachycardia
