
Page 917 - TNFlipTest
P. 917
Toronto Notes 2019 Glaucoma Secondary Open Angle Glaucoma
• increasedIOPsecondarytoocular/systemicdisordersthatobstructthetrabecularmeshwork ■ steroid-induced glaucoma
■ traumatic glaucoma
■ pigmentary dispersion syndrome
■ pseudoexfoliationsyndrome
Primary Angle-Closure Glaucoma
• 5%ofallglaucomacases
• peripheralirisbowsforwardobstructingaqueousaccesstothetrabecularmeshwork
• suddenforwardshiftofthelens-irisdiaphragmcausespupillaryblockandresultsinimpaireddrainage,
leading to a sudden rise in IOP
Risk Factors
• hyperopia:smalleye,biglens–largelenscrowdstheangle • age>70yr
• female
• familyhistory
• morecommoninpeopleofAsianandInuitdescent
• maturecataracts
• shallowanteriorchamber
• pupildilation(topicalandsystemicanticholinergics,stress,darkness)
Clinical Features
• red,painfuleye=REDFLAG
• unilateral,butothereyeatincreasedrisk
• decreasedvisualacuity,visionacutelyblurredfromcornealedema
• halosaroundlights
• nauseaandvomiting,abdominalpain
• fixed,mid-dilatedpupil
• markedincreaseinIOP;maybenoticeableeventopalpation(>40mmHg) • shallowanteriorchamber±cellsinanteriorchamber
Complications
• irreversiblelossofvisionwithinhourstodaysifuntreated
• permanentperipheralanteriorsynechiae,resultinginpermanentangleclosure
Treatment
• OCULAREMERGENCY:refertoophthalmologistforacuteangleclosureglaucoma • medicaltreatment(seeGlaucomaMedications,Table14,OP42)
■ aqueous suppressants and hyperosmotic agents
■ miotic drops (pilocarpine) to reverse pupillary block
■ multiple topical IOP-lowering agents
■ hypserosmotic agents such as oral glycerine, or IV mannitol
• laseriridotomyisdefinitive
Secondary Angle-Closure Glaucoma
Uveitis
• inflamedirisadherestolens(posteriorsynechiae)
Neovascular Glaucoma
• abnormalbloodvesselsdeveloponsurfaceofiris(rubeosisiridis),intheangle,andwithinthe trabecular meshwork
• duetoretinalischemiaassociatedwithPDRorCRVO
• treatmentwithlasertherapytoretinareducesneovascularstimulustoirisandanglevessels
Ophthalmology OP27
Rule of Fours
1/4 of general population using topical steroid for 4 wk, 4x/d will develop an increase in IOP
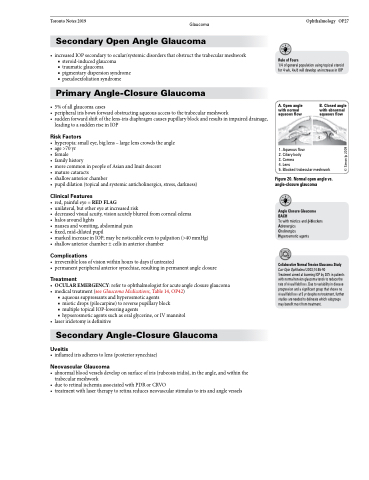
A. Open angle with normal aqueous flow
2
1
1. Aqueous flow 2. Ciliary body 3. Cornea
4. Lens
3
B. Closed angle with abnormal aqueous flow
5
Collaborative Normal Tension Glaucoma Study
Curr Opin Ophthalmol 2003;14:86-90
Treatment aimed at lowering IOP by 30% in patients with normal tension glaucoma tends to reduce the rate of visual field loss. Due to variability in disease progression and a significant group that shows no visual field loss at 5 yr despite no treatment, further studies are needed to delineate which subgroups may benefit most from treatment.
4
5. Blocked trabecular meshwork
Figure20.Normalopenanglevs. angle-closureglaucoma
Angle Closure Glaucoma BACH
Tx with miotics and β-blockers Adrenergics
Cholinergics
Hyperosmotic agents
© Simon Ip 2009
