
Page 1051 - TNFlipTest
P. 1051
Toronto Notes 2019 Cardiology Pediatrics P17
Investigations
• Echo, ECG, CXR
• preandpostductaloxygensaturations,4limbBPs,hyperoxiatest
CYANOTIC VS . ACYANOTIC CONGENITAL HEART DISEASE
• cyanosis:bluemucousmembranes,nailbeds,andskinsecondarytoanabsoluteconcentrationof deoxygenated hemoglobin of at least 30 g/dL
• acyanoticheartdisease(i.e.LtoRshunt,obstructionoccurringbeyondlungs):bloodpassesthrough pulmonic circulation → oxygenation takes place → low levels of deoxygenated blood in systemic circulation → no cyanosis
• cyanoticheartdisease(i.e.RtoLshunt):bloodbypassesthelungs→nooxygenationoccurs→high levels of deoxygenated hemoglobin enters the systemic circulation → cyanosis
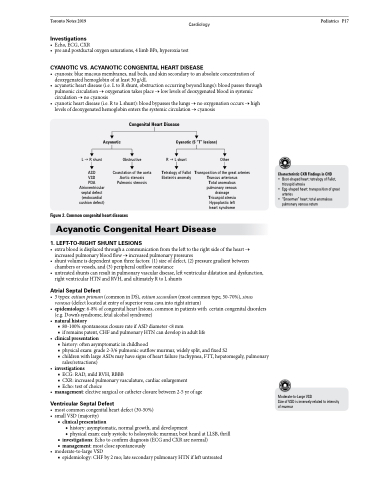
Acyanotic
Congenital Heart Disease
Cyanotic (5 “T” lesions)
LR shunt ASD
VSD
PDA Atrioventricular septal defect (endocardial cushion defect)
Obstructive
Coarctation of the aorta Aortic stenosis Pulmonic stenosis
RL shunt Tetralogy of Fallot
Ebstein’s anomaly
Other Transposition of the great arteries
Truncus arteriosus Total anomalous pulmonary venous drainage Tricuspid atresia Hypoplastic left heart syndrome
Characteristic CXR Findings in CHD
• Boot-shaped heart: tetralogy of Fallot, tricuspid atresia
• Egg-shaped heart: transposition of great arteries
• “Snowman” heart: total anomalous pulmonary venous return
Figure 2. Common congenital heart diseases
Acyanotic Congenital Heart Disease
1 . LEFT-TO-RIGHT SHUNT LESIONS
• extrabloodisdisplacedthroughacommunicationfromthelefttotherightsideoftheheart→ increased pulmonary blood flow → increased pulmonary pressures
• shuntvolumeisdependentuponthreefactors:(1)sizeofdefect,(2)pressuregradientbetween chambers or vessels, and (3) peripheral outflow resistance
• untreatedshuntscanresultinpulmonaryvasculardisease,leftventriculardilatationanddysfunction, right ventricular HTN and RVH, and ultimately R to L shunts
Atrial Septal Defect
• 3types:ostiumprimum(commoninDS),ostiumsecundum(mostcommontype,50-70%),sinus venosus (defect located at entry of superior vena cava into right atrium)
• epidemiology: 6-8% of congenital heart lesions, common in patients with certain congenital disorders (e.g. Down’s syndrome, fetal alcohol syndrome)
• naturalhistory
■ 80-100% spontaneous closure rate if ASD diameter <8 mm
■ if remains patent, CHF and pulmonary HTN can develop in adult life
• clinicalpresentation
■ history: often asymptomatic in childhood
■ physical exam: grade 2-3/6 pulmonic outflow murmur, widely split, and fixed S2
■ children with large ASDs may have signs of heart failure (tachypnea, FTT, hepatomegaly, pulmonary
rales/retractions)
• investigations
■ ECG: RAD, mild RVH, RBBB
■ CXR: increased pulmonary vasculature, cardiac enlargement ■ Echo: test of choice
• management:electivesurgicalorcatheterclosurebetween2-5yrofage
Ventricular Septal Defect
• mostcommoncongenitalheartdefect(30-50%) • smallVSD(majority)
■ clinical presentation
◆ history: asymptomatic, normal growth, and development
◆ physical exam: early systolic to holosystolic murmur, best heard at LLSB, thrill
■ investigations:Echotoconfirmdiagnosis(ECGandCXRarenormal)
■ management: most close spontaneously • moderate-to-largeVSD
Moderate-to-Large VSD
Size of VSD is inversely related to intensity of murmur
■ epidemiology: CHF by 2 mo; late secondary pulmonary HTN if left untreated
