
Page 641 - TNFlipTest
P. 641
Toronto Notes 2019
Flatworms
Infectious Diseases ID41
Flatworms
Cestodes/Trematodes
Table 27. Cestodes/Trematodes (Flatworms)
CESTODES
Taenia solium
Taenia saginata Diphyllobothrium latum
Echinococcus granulosus
TREMATODES
Clonorchis sinensis Schistosoma spp.
Epidemiology
Developing countries
Developing countries Europe, North America, Asia
Rural areas, Sheep-raising countries
Japan, Taiwan, China, SE Asia
Africa, SE Asia, focal in Western Hemisphere
Transmission
Undercooked pork (larvae), human feces (eggs)
Undercooked beef (larvae) Raw fish
Dog feces (eggs)
Raw fish
Fresh water exposure
Medical Importance
Taeniasis: mild abdominal symptoms
Cysticercosis: mass lesions in CNS, eyes, skin, seizures
Mild GI symptoms
B12 deficiency leading to macrocytic anemia and posterior column deficits
Liver/lung cysts (enlarge between 1-20 yr; may cause mass effect or rupture)
Risk of anaphylaxis if cystic
fluid released during surgical evacuation
Exists in bile ducts, causes inflammation and sometimes cholangiocarcinoma
Chronic sequelae secondary to long-term infection (e.g. chronic liver disease, SCC of the bladder)
Treatment
Corticosteroids + albendazole for cysticercosis
Antiepileptics if seizures Praziquantel for adult tapeworm in gut (taeniasis)
Praziquantel Praziquantel
Albendazole ± praziquantel alone Surgery + perioperative albendazole
Percutaneous aspiration + perioperative albendazole
Praziquantel Praziquantel
Schistosoma spp.
Etiology
• infectionwithSchistosomaspp.(S.mansoni,S.hematobium,S.japonicum)occursfollowingpenetration of unbroken skin by their larvae (cercariae) which are found in infested fresh water
• adult worms live in terminal venules of bladder/bowel passing eggs into urine/stool
• eggsmustreachfreshwatertohatchwheretheyinfectanintermediatehost(snails)whichthenrelease
cercariae into the water
• schistosomescannotmultiplyinorpassbetweenhumans
• morecommoninindividualsfromsub-SaharanAfrica,SouthAmerica,Asia,Caribbean,Eastern
Mediterranean/North Africa
Clinical Presentation
• mostasymptomatic;symptomsseenintravellers(nonimmune)
• swimmer’sitch:pruriticskinrashatsiteofpenetration(cercarialdermatitis)
• acuteschistosomiasis(Katayamafever):hypersensitivitytomigratingparasites(4-8wkafterinfection)
■ fever, hives, headache, weight loss, cough, abdominal pain, chronic diarrhea, high-grade eosinophilia
• chronicschistosomiasis(canpersistforyears): ■ S. mansoni, S. japonicum
◆ worms in mesenteric vein, eggs in portal tracts of liver and bowel
◆ heavy infections: intestinal polyps, portal and pulmonary HTN, splenomegaly (2o to portal
HTN), hepatomegaly
■ S. hematobium
◆ worms in vesical plexus, eggs in distal ureter and bladder induce granulomas and fibrosis
◆ hematuria and obstructive uropathy; associated with squamous cell bladder cancer
■ neurologic complications: spinal cord neuroschistosomiasis (transverse myelitis), cerebral or
cerebellar neuroschistosomiasis (increased ICP, focal CNS signs, seizures)
■ pulmonary complications: granulomatous pulmonary endarteritis, pulmonary HTN, cor
pulmonale; especially in patients with hepatosplenic involvement
Investigations
• serology(highsensitivityandspecificity),CBC(eosinophilia,anemia,thrombocytopenia)
• S.mansoni,S.japonicum:eggsinstool,liverU/Sshowsfibrosis,rectalbiopsy
• S.hematobium:bladderbiopsy,eggsinurineandoccasionallystool,kidneyandbladderU/S
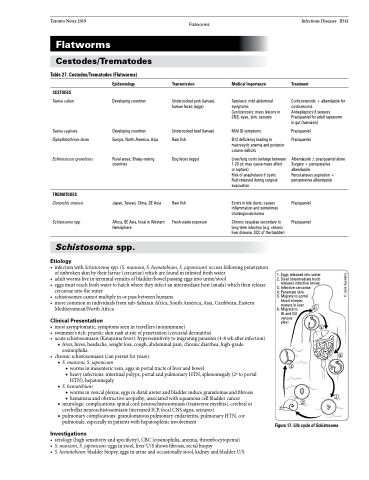
1. Eggs released into water 2. Snail (intermediate host) releases infective larvae
3. Infective cercariae 4. Penetrate skin
5. Migrate to portal
blood stream;
mature in liver 6. Migrate to
GI and GU venous plexi
3
5
4
6
1
2
Figure 17. Life cycle of Schistosoma
© Julie Saunders
