
Page 674 - TNFlipTest
P. 674
MI6 Medical Imaging Chest Imaging
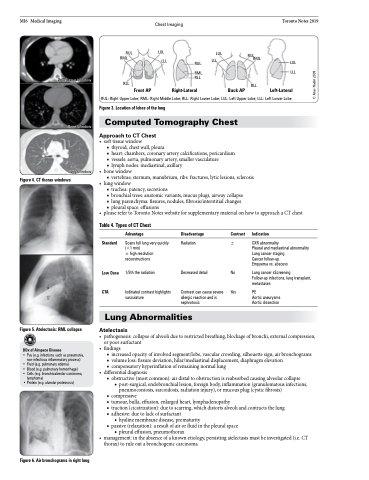
RUL LUL LUL
RUL RML
Toronto Notes 2019
LUL LLL
Soft Tissue Window
Bone Window
Lung Window
RML LLL RUL LLL
RML RLL
RLL
RUL: Right Upper Lobe; RML: Right Middle Lobe; RLL: Right Lower Lobe; LUL: Left Upper Lobe; LLL: Left Lower Lobe
Figure 3. Location of lobes of the lung
Computed Tomography Chest
Approach to CT Chest
• softtissuewindow
■ thyroid, chest wall, pleura
■ heart: chambers, coronary artery calcifications, pericardium ■ vessels: aorta, pulmonary artery, smaller vasculature
■ lymph nodes: mediastinal, axillary
• bonewindow
■ vertebrae, sternum, manubrium, ribs: fractures, lytic lesions, sclerosis
• lungwindow
■ trachea: patency, secretions
■ bronchial trees: anatomic variants, mucus plugs, airway collapse ■ lung parenchyma: fissures, nodules, fibrosis/interstitial changes ■ pleural space: effusions
• pleaserefertoTorontoNoteswebsiteforsupplementarymaterialonhowtoapproachaCTchest
Front AP Right-Lateral
Back AP
RLL
Left-Lateral
Figure 4. CT thorax windows
Table 4. Types of CT Chest
Standard
Low Dose CTA
Advantage
Scans full lung very quickly (<1 min)
± high resolution reconstructions
1/5th the radiation
Iodinated contrast highlights vasculature
Disadvantage Contrast
Radiation ±
Indication
CXR abnormality
Pleural and mediastinal abnormality Lung cancer staging
Cancer follow-up
Empyema vs. abscess
Lung cancer sScreening
Follow-up infections, lung transplant, metastases
PE
Aortic aneurysms Aortic dissection
Decreased detail
Contrast can cause severe allergic reaction and is nephrotoxic
No Yes
Figure 5. Atelectasis: RML collapse
DDx of Airspace Disease
Lung Abnormalities
Atelectasis
• pathogenesis:collapseofalveoliduetorestrictedbreathing,blockageofbronchi,externalcompression,
• Pus (e.g. infections such as pneumonia, non-infectious inflammatory process)
• Fluid (e.g. pulmonary edema)
• Blood (e.g. pulmonary hemorrhage)
• Cells (e.g. bronchioalveolar carcinoma,
lymphoma)
• Protein (e.g. alveolar proteinosis)
•
•
•
or poor surfactant findings
■ increased opacity of involved segment/lobe, vascular crowding, silhouette sign, air bronchograms ■ volume loss: fissure deviation, hilar/mediastinal displacement, diaphragm elevation
■ compensatory hyperinflation of remaining normal lung
differentialdiagnosis
■ obstructive (most common): air distal to obstruction is reabsorbed causing alveolar collapse
◆ post-surgical, endobronchial lesion, foreign body, inflammation (granulomatous infections, pneumoconiosis, sarcoidosis, radiation injury), or mucous plug (cystic fibrosis)
■ compressive
■ tumour, bulla, effusion, enlarged heart, lymphadenopathy
■ traction (cicatrization): due to scarring, which distorts alveoli and contracts the lung ■ adhesive: due to lack of surfactant
◆ hyaline membrane disease, prematurity
■ passive (relaxation): a result of air or fluid in the pleural space
◆ pleural effusion, pneumothorax management:intheabsenceofaknownetiology,persistingatelectasismustbeinvestigated(i.e.CT thorax) to rule out a bronchogenic carcinoma
Figure 6. Air bronchograms in right lung
© Anas Nader 2009
