
Page 947 - TNFlipTest
P. 947
Toronto Notes 2019
Shoulder
Orthopedics OR13
© Andreea Margineanu 2012
© Lori Waters 2005 © Lori Waters 2005
© Tabby Lulham 2010
Anterior apprehension sign
Posterior apprehension sign
Figure 12. Shoulder maneuvers
Rotator Cuff Disease
© Lori Waters 2005
Sulcus sign
Traction-Countertraction
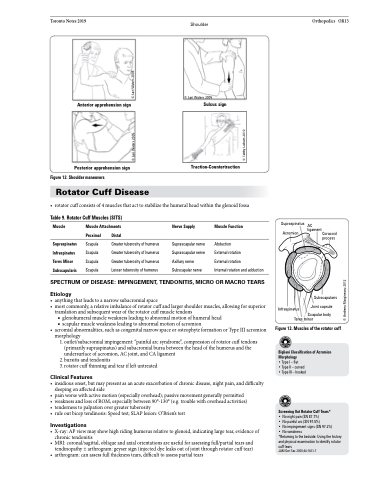
• rotatorcuffconsistsof4musclesthatacttostabilizethehumeralheadwithintheglenoidfossa
Table 9. Rotator Cuff Muscles (SITS)
Muscle
Supraspinatus Infraspinatus Teres Minor Subscapularis
Muscle Attachments
Nerve Supply
Suprascapular nerve Suprascapular nerve Axillary nerve Subscapular nerve
Muscle Function
Abduction
External rotation
External rotation
Internal rotation and adduction
Supraspinatus AC
Proximal
Scapula Scapula Scapula Scapula
Distal
Greater tuberosity of humerus Greater tuberosity of humerus Greater tuberosity of humerus Lesser tuberosity of humerus
Acromion
Infraspinatus
Teres minor
SPECTRUM OF DISEASE: IMPINGEMENT, TENDONITIS, MICRO OR MACRO TEARS
Etiology
• anythingthatleadstoanarrowsubacromialspace
• most commonly, a relative imbalance of rotator cuff and larger shoulder muscles, allowing for superior
translation and subsequent wear of the rotator cuff muscle tendons
■ glenohumeral muscle weakness leading to abnormal motion of humeral head ■ scapularmuscleweaknessleadingtoabnormalmotionofacromion
• acromialabnormalities,suchascongenitalnarrowspaceorosteophyteformationorTypeIIIacromion morphology
1. outlet/subacromial impingement: “painful arc syndrome”, compression of rotator cuff tendons (primarily supraspinatus) and subacromial bursa between the head of the humerus and the undersurface of acromion, AC joint, and CA ligament
2. bursitis and tendonitis
3. rotator cuff thinning and tear if left untreated
Clinical Features
• insidiousonset,butmaypresentasanacuteexacerbationofchronicdisease,nightpain,anddifficulty sleeping on affected side
• painworsewithactivemotion(especiallyoverhead);passivemovementgenerallypermitted
• weaknessandlossofROM,especiallybetween90°-130°(e.g.troublewithoverheadactivities)
• tendernesstopalpationovergreatertuberosity
• ruleoutbiceptendinosis:Speedtest;SLAPlesion:O’Brien’stest
Investigations
• X-ray:APviewmayshowhighridinghumerusrelativetoglenoid,indicatinglargetear,evidenceof chronic tendonitis
• MRI:coronal/sagittal,obliqueandaxialorientationsareusefulforassessingfull/partialtearsand tendinopathy ± arthrogram: geyser sign (injected dye leaks out of joint through rotator cuff tear)
• arthrogram:canassessfullthicknesstears,difficulttoassesspartialtears
Scapular body
ligament Coracoid process
Subscapularis Joint capsule
Figure13.Musclesoftherotatorcuff
Bigliani Classification of Acromion Morphology
•TypeI–flat
• Type II – curved
• Type III – hooked
Screening Out Rotator Cuff Tears*
• No night pain (SN 87.7%)
• No painful arc (SN 97.5%)
• No impingement signs (SN 97.2%)
• No weakness
*Returning to the bedside: Using the history and physical examination to identify rotator
cuff tears
JAM Geri Soc 2000;48:1633-7
