
Page 1337 - TNFlipTest
P. 1337
Toronto Notes 2019
Stone Disease
Urology U19
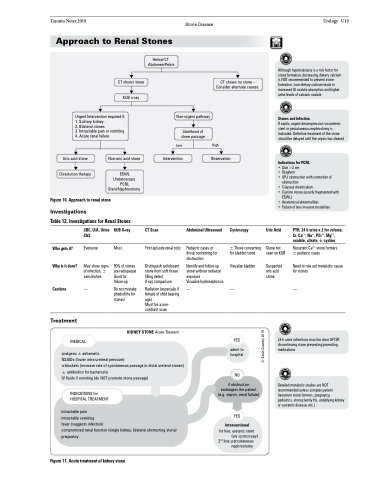
Approach to Renal Stones
Helical CT Abdomen/Pelvis
CT shows stone KUB x-ray
Urgent Intervention required if: 1. Solitary kidney
2. Bilateral stones
3. Intractable pain or vomiting 4. Acute renal failure
Non-urgent pathway
Likelihood of stone passage
CT shows no stone – Consider alternate causes
High Observation
Although hypercalciuria is a risk factor for stone formation, decreasing dietary calcium is NOT recommended to prevent stone formation. Low dietary calcium leads to increased GI oxalate absorption and higher urine levels of calcium oxalate
Stones and Infection
If septic, urgent decompression via ureteric stent or percutaneous nephrostomy is indicated. Definitive treatment of the stone should be delayed until the sepsis has cleared
Indications for PCNL
Uric acid stone
Dissolution therapy
Non-uric acid stone
ESWL Ureteroscopy PCNL Stent/Nephrostomy
Low Intervention
CT Scan
First episode renal colic
Distinguish radiolucent stone from soft tissue filling defect
X-ray comparison
Size >2 cm
Staghorn
UPJ obstruction with correction of obstruction
Calyceal diverticulum
Cystine stones (poorly fragmented with ESWL)
Anatomical abnormalities
Failure of less invasive modalities
Figure 10. Approach to renal stone
Investigations
Table 12. Investigations for Renal Stones
• • •
• •
• •
Uric Acid
Stone not seen on KUB
Suspected uric acid stone
24 h urine collections must be done AFTER discontinuing stone preventing/promoting medications
Detailed metabolic studies are NOT recommended unless complex patient (recurrent stone formers, pregnancy, pediatrics, strong family Hx, underlying kidney or systemic disease, etc.)
Who gets it? Why is it done?
Cautions
Treatment
Radiation (especially if — female of child bearing
age)
Must be a non-
contrast scan
Cystoscopy
± Those concerning for bladder stone
Visualize bladder
—
YES
admit to hospital
NO
if obstruction endangers the patient (e.g. sepsis, renal failure)
YES
Interventional
1st line: ureteric stent (via cystoscopy)
2nd line: percutaneous nephrostomy
PTH, 24 h urine x 2 for volume, Cr, Ca2+, Na+, PO43–, Mg2+, oxalate, citrate, ± cystine
Recurrent Ca2+ stone formers ± pediatric cases
Need to rule out metabolic cause for stones
—
CBC, U/A, Urine C&S
Everyone
May show signs of infection, ± sensitivities
—
KUB X-ray
Most
90% of stones are radiopaque Good for follow-up
Do not mistake phleboliths for stones!
Abdominal Ultrasound
Pediatric cases or those concerning for obstruction
Identify and follow-up stone without radiation exposure
Visualize hydronephrosis
KIDNEY STONE Acute Treatent
MEDICAL
analgesic + antiemetic
NSAIDs (lower intra-ureteral pressure)
α-blockers (increase rate of spontaneous passage in distal ureteral stones) + antibiotics for bacteriuria
IV fluids if vomiting (do NOT promote stone passage)
INDICATIONS for HOSPITAL TREATMENT
intractable pain
intractable vomiting
fever (suggests infection)
compromised renal function (single kidney, bilateral obstructing stone) pregnancy
Figure 11. Acute treatment of kidney stone
© Sarah Crawley 2019
