
Page 1338 - TNFlipTest
P. 1338
U20 Urology
Stone Disease
Toronto Notes 2019
Alpha-blockers as Medical Expulsive Therapy for Ureteral Stones
Cochrane DB Syst Rev 2014;4:CD008509 Purpose: To determine whether or
not α-blockers compared with other pharmacological treatments or placebo improve stone clearance rates and other clinically relevant outcomes in patients presenting with symptoms of stones less than 10 mm confirmed by imaging. Results/Conclusions: 32 RCTs, 5,864 participants. Although patients using α-blockers were more likely to experience adverse effects compared to standard therapy, stone-free rates were significantly higher in the α-blocker group (RR 1.48, 95% CI 1.33-1.64), expulsion time was 2.91 days shorter, and there was a reduction in the number of pain episodes (MD -0.48, 95%
CI -0.94 to -0.01), the need for analgesic medication (MD -38.17, 95% CI -74.93 to -1.41), and hospitalization (RR 0.35, 95% CI 0.13-0.97). α-blockers should therefore be offered as a primary treatment modality for ureteral stones.
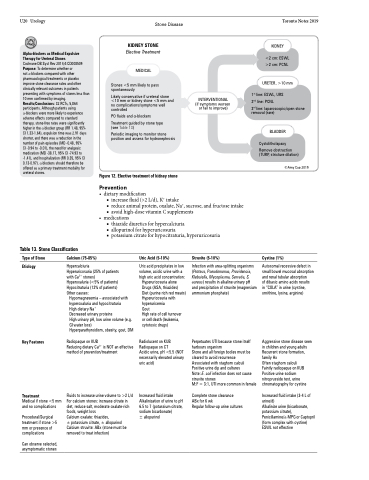
KIDNEY STONE
Elective Treatment
MEDICAL
Stones <5 mm likely to pass spontaneously
Likely conservative if ureteral stone <10 mm or kidney stone <5 mm and no complications/symptoms well controlled
PO fluids and α-blockers Treatment guided by stone type
(see Table 13)
Periodic imaging to monitor stone
position and assess for hydronephrosis
Figure 12. Elective treatment of kidney stone
Prevention
INTERVENTIONAL (if symptoms worsen or fail to improve)
KIDNEY
<2 cm: ESWL >2 cm: PCNL
URETER, >10 mm
1st line: ESWL, URS 2nd line: PCNL
3rd line: laparoscopic/open stone removal (rare)
BLADDER
Cystolitholapaxy
Remove obstruction (TURP, stricture dilation)
©Amy Cao 2019
Table 13. Stone Classification
Type of Stone
Etiology
Calcium (75-85%)
Hypercalciuria
Hyperuricosuria (25% of patients with Ca2+ stones)
Hyperoxaluria (<5% of patients) Hypocitraturia (12% of patients) Other causes:
Hypomagnesemia – associated with hyperoxaluria and hypocitraturia High dietary Na+
Decreased urinary proteins
High urinary pH, low urine volume (e.g. GI water loss)
Hyperparathyroidism, obesity, gout, DM
Radiopaque on KUB
Reducing dietary Ca2+ is NOT an effective method of prevention/treatment
Fluids to increase urine volume to >2 L/d For calcium stones: increase citrate in diet, reduce salt, moderate oxalate-rich foods, weight loss
Calcium oxalate: thiazides,
± potassium citrate, ± allopurinol Calcium struvite: ABx (stone must be removed to treat infection)
Uric Acid (5-10%)
Uric acid precipitates in low volume, acidic urine with a high uric acid concentration:
Hyperuricosuria alone Drugs (ASA, thiazides) Diet (purine rich red meats) Hyperuricosuria with hyperuricemia
Gout
High rate of cell turnover or cell death (leukemia, cytotoxic drugs)
Radiolucent on KUB Radiopaque on CT
Acidic urine, pH <5.5 (NOT necessarily elevated urinary uric acid)
Increased fluid intake Alkalinization of urine to pH 6.5 to 7 (potassium citrate, sodium bicarbonate)
± allopurinol
Struvite (5-10%)
Infection with urea-splitting organisms (Proteus, Pseudomonas, Providencia, Klebsiella, Mycoplasma, Serratia, S. aureus) results in alkaline urinary pH and precipitation of struvite (magnesium ammonium phosphate)
Perpetuates UTI because stone itself harbours organism
Stone and all foreign bodies must be cleared to avoid recurrence Associated with staghorn calculi Positive urine dip and cultures
Note: E. coli infection does not cause struvite stones
M:F = 3:1, UTI more common in female
Complete stone clearance
ABx for 6 wk
Regular follow-up urine cultures
Cystine (1%)
Autosomal recessive defect in small bowel mucosal absorption and renal tubular absorption
of dibasic amino acids results in “COLA” in urine (cystine, ornithine, lysine, arginine)
Aggressive stone disease seen in children and young adults Recurrent stone formation, family Hx
Often staghorn calculi Faintly radiopaque on KUB Positive urine sodium nitroprusside test, urine chromatography for cystine
Increased fluid intake (3-4 L of urine/d)
Alkalinize urine (bicarbonate, potassium citrate), Penicillamine/α-MPG or Captopril (form complex with cystine) ESWL not effective
• dietarymodification
■ increase fluid (>2 L/d), K+ intake
■ reduce animal protein, oxalate, Na+, sucrose, and fructose intake ■ avoid high-dose vitamin C supplements
• medications
■ thiazide diuretics for hypercalciuria
■ allopurinol for hyperuricosuria
■ potassium citrate for hypocitraturia, hyperuricosuria
Key Features
Treatment
Medical if stone <5 mm and no complications
Procedural/Surgical treatment if stone >5 mm or presence of complications
Can observe selected, asymptomatic stones
