
Page 1342 - TNFlipTest
P. 1342
U24 Urology
Urological Neoplasms
Toronto Notes 2019
Radiotherapy With or Without Chemotherapy in Muscle-Invasive Bladder Cancer
NEJM 2012;366:1477-1488
Study: Phase 3 trial with random assignment of 360 patients with muscle-invasive bladder cancer to radiotherapy with or without chemotherapy. Results: At 2 yr, rates of locoregional disease-free survival were 67% in the chemoradiotherapy group and 54% in the radiotherapy group (HR 0.68, 95% CI 0.48-0.96). Five year overall survival rates were 48% in the chemoradiotherapy group and 35% in the radiotherapy group (HR 0.82, 95% CI 0.63-1.09). Conclusions: Chemotherapy with fluorouracil and mitomycin C in combination with radiotherapy improves locoregional control of bladder cancer compared to radiotherapy alone, with no significant increase in adverse events.
Investigations
• CTurogram
• cystoscopyandretrogradepyelogram
Treatment
• radicalnephroureterectomywithexcisionofipsilateralbladdercuff
• distalureterectomyfordistalureteraltumourswithconcomitantureteralreimplant
• segmentalresectionwithuretero-ureterostomyforsomemid-ureteraltumoursisalsodone
• emergingroleforendoscopiclaserablationinpatientswithlowgradedisease,poorbaselinerenalhealth
Bladder Carcinoma
Etiology
• unknown,butenvironmentalriskfactorsinclude:
■ smoking (main factor – implicated in 60% of new cases)
■ aromatic amines: naphthylamines, benzidine, tryptophan, phenacetin metabolites
■ cyclophosphamide
■ prior Hx of radiation treatment to the pelvis
■ Schistosoma hematobium infection (associated with SCC)
■ chronic irritation: cystitis, chronic catheterization, bladder stones (associated with SCC)
■ aristolochic acid: associated with Balkan Nephropathy (renal failure, upper tract urothelial cancer)
and Chinese Herbal Nephropathy
Epidemiology
• 2ndmostcommonurologicalmalignancy
• M:F=3:1,morecommonamongwhitesthanblacks • meanageatdiagnosisis65yr
Pathology
• classification
■ urothelial carcinoma (UC) >90% ■ SCC5-7%
■ adenocarcinoma 1%
■ others <1%
• stagesandprognosesofurothelialcarcinomaatdiagnosis ■ non-muscle invasive (75%) → >80% overall survival
◆ 15% of these will progress to invasive UC
◆ majority of these patients will have recurrence ■ invasive(25%)→50-60%5yrsurvival
◆ 85% have no prior history of superficial UC (i.e. de novo)
◆ 50% have occult metastases at diagnosis, and most of these will develop overt clinical evidence
of metastases within 1 yr – lymph nodes, lung, peritoneum, liver
• carcinomainsitu→flat,non-papillaryerythematouslesioncharacterizedbydysplasiaconfinedto
urothelium
■ more aggressive, worse prognosis ■ usually multifocal
■ may progress to invasive UCC
Clinical Features
• asymptomatic (20%)
• hematuria(keysymptom:85-90%atthetimeofdiagnosis)
• pain(50%)→locationdeterminedbysize/extentoftumour(i.e.flank,suprapubic,perineal,abdominal,etc.) • clot retention (17%)
• storageurinarysymptoms→considercarcinomainsitu
• palpablemassonbimanualexam→likelymuscleinvasion
• obstructionofureters→hydronephrosisanduremia(nausea,vomiting,anddiarrhea)
Investigations
• U/A,urineC&S,urinecytology
• U/S
• CTscanwithcontrast→lookforfillingdefectsinuppertracts
• cystoscopywithbiopsy(ifsmalllesion)
• TURBT(goldstandard,diagnosticandoftentherapeutic)→establishdiagnosisanddeterminedepthof
penetration
• specificbladdertumourmarkers(e.g.NMP-22,BTA,Immunocyt,FDP);utilityinclinicalpractice
debatable)
Grading
• low grade: <=10% invasive, 60% recur locally
• highgrade:50-80%areinvasiveorareexpectedtoprogresstoinvasiveovertime
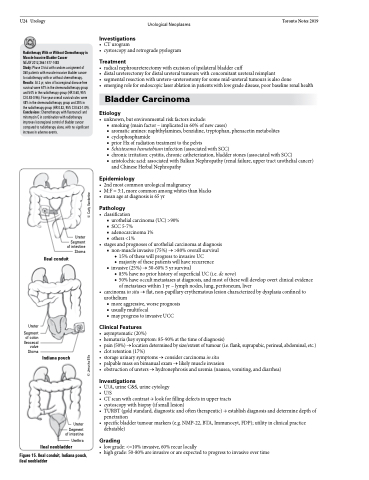
Ureter Segment of intestine Stoma
Ileal conduit
Ureter
Segment of colon Ileocecal
valve Stoma
Indiana pouch
Ureter
Segment of intestine
Urethra
Ileal neobladder
Figure 15. Ileal conduit, Indiana pouch, ileal neobladder
© Jerusha Ellis © Carly Vanderlee
