
Page 940 - TNFlipTest
P. 940
OR6 Orthopedics
Fractures – General Principles
Toronto Notes 2019
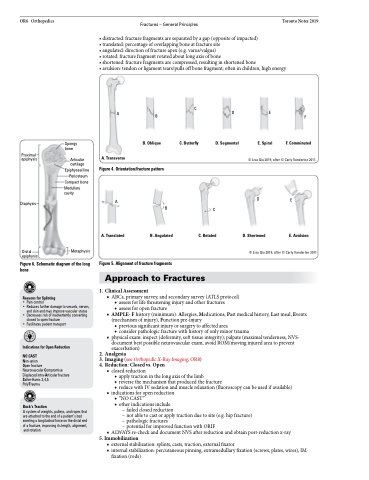
• distracted: fracture fragments are separated by a gap (opposite of impacted) • translated: percentage of overlapping bone at fracture site
• angulated: direction of fracture apex (e.g. varus/valgus)
• rotated: fracture fragment rotated about long axis of bone
• shortened: fracture fragments are compressed, resulting in shortened bone
• avulsion: tendon or ligament tears/pulls off bone fragment; often in children, high energy
Spongy bone
Articular cartilage
Epiphyseal line Periosteum Compact bone
Medullary cavity
Metaphysis
D. Segmental
E. Spiral
A
A. Transverse
B
B. Oblique
C
C. Butterfly
DE
F
F. Comminuted
Proximal epiphysis
Diaphysis
Distal epiphysis
© Lisa Qiu 2019, after © Carly Vanderlee 2011
Figure 4. Orientation/fracture pattern
A
A. Translated
B
B. Angulated
C
D
D. Shortened
E
E. Avulsion
C. Rotated
© Lisa Qiu 2019, after © Carly Vanderlee 2011
Figure 6. Schematic diagram of the long bone
Reasons for Splinting
• Pain control
• Reduces further damage to vessels, nerves,
and skin and may improve vascular status
• Decreases risk of inadvertently converting
closed to open fracture
• Facilitates patient transport
Indications for Open Reduction NO CAST
Non-union
Open fracture
Neurovascular Compromise Displaced intra-Articular fracture Salter-Harris 3,4,5
PolyTrauma
Buck’s Traction
A system of weights, pulleys, and ropes that are attached to the end of a patient’s bed exerting a longitudinal force on the distal end of a fracture, improving its length, alignment,
and rotation
Figure 5. Alignment of fracture fragments
1.
2. 3. 4.
Approach to Fractures
Clinical Assessment
■ ABCs, primary survey, and secondary survey (ATLS protocol) ◆ assess for life threatening injury and other fractures
◆ assess for open fracture
■ AMPLE- F history (minimum): Allergies, Medications, Past medical history, Last meal, Events (mechanism of injury), Function pre-injury
◆ previous significant injury or surgery to affected area
◆ consider pathologic fracture with history of only minor trauma
■ physical exam: inspect (deformity, soft tissue integrity); palpate (maximal tenderness, NVS-
document best possible neurovascular exam, avoid ROM/moving injured area to prevent
exacerbation)
Analgesia
Imaging (see Orthopedic X-Ray Imaging, OR8) Reduction: Closed vs. Open
■ closed reduction
◆ apply traction in the long axis of the limb
◆ reverse the mechanism that produced the fracture
◆ reduce with IV sedation and muscle relaxation (fluoroscopy can be used if available)
■ indications for open reduction ◆ “NO CAST”
◆ other indications include
– failed closed reduction
– not able to cast or apply traction due to site (e.g. hip fracture) – pathologic fractures
– potential for improved function with ORIF
■ ALWAYS re-check and document NVS after reduction and obtain post-reduction x-ray
5. Immobilization
■ external stabilization: splints, casts, traction, external fixator
■ internal stabilization: percutaneous pinning, extramedullary fixation (screws, plates, wires), IM
fixation (rods)
