
Page 97 - TNFlipTest
P. 97
Toronto Notes 2019
Ischemic Heart Disease
Cardiology and Cardiac Surgery C29
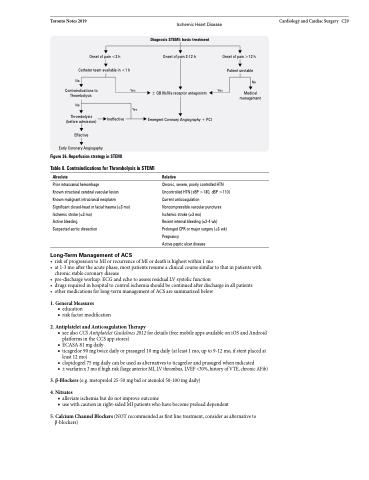
Onset of pain <3 h
Catheter team available in <1 h No
Contraindications to Yes Thrombolysis
Diagnosis STEMI: basic treatment
Onset of pain 3-12 h
± GB IIb/IIIa receptor antagonists
Emergent Coronary Angiography + PCI
Onset of pain >12 h
Patient unstable
No
Yes Medical management
No
Thrombolysis (before admission)
Effective
Early Coronary Angiogaphy
Yes
Ineffective
Figure 36. Reperfusion strategy in STEMI
Table 8. Contraindications for Thrombolysis in STEMI
Absolute
Prior intracranial hemorrhage
Known structural cerebral vascular lesion Known malignant intracranial neoplasm Significant closed-head or facial trauma (≤3 mo) Ischemic stroke (≤3 mo)
Active bleeding
Suspected aortic dissection
Long-Term Management of ACS
Relative
Chronic, severe, poorly controlled HTN Uncontrolled HTN (sBP >180, dBP >110) Current anticoagulation
Noncompressible vascular punctures Ischemic stroke (≥3 mo)
Recent internal bleeding (≤2-4 wk) Prolonged CPR or major surgery (≤3 wk) Pregnancy
Active peptic ulcer disease
• riskofprogressiontoMIorrecurrenceofMIordeathishighestwithin1mo
• at1-3moaftertheacutephase,mostpatientsresumeaclinicalcoursesimilartothatinpatientswith
chronic stable coronary disease
• pre-dischargeworkup:ECGandechotoassessresidualLVsystolicfunction
• drugsrequiredinhospitaltocontrolischemiashouldbecontinuedafterdischargeinallpatients
• othermedicationsforlong-termmanagementofACSaresummarizedbelow
1. General Measures
■ education
■ risk factor modification
2. Antiplatelet and Anticoagulation Therapy
■ see also CCS Antiplatelet Guidelines 2012 for details (free mobile apps available on iOS and Android platforms in the CCS app stores)
■ ECASA81mgdaily
■ ticagrelor 90 mg twice daily or prasugrel 10 mg daily (at least 1 mo, up to 9-12 mo, if stent placed at
least 12 mo)
■ clopidogrel 75 mg daily can be used as alternatives to ticagrelor and prasugrel when indicated
■ ±warfarinx3moifhighrisk(largeanteriorMI,LVthrombus,LVEF<30%,historyofVTE,chronicAFib)
3. β-Blockers (e.g. metoprolol 25-50 mg bid or atenolol 50-100 mg daily)
4. Nitrates
■ alleviate ischemia but do not improve outcome
■ use with caution in right-sided MI patients who have become preload dependent
5. Calcium Channel Blockers (NOT recommended as first line treatment, consider as alternative to β-blockers)
