
Page 688 - TNFlipTest
P. 688
MI20 Medical Imaging
Neuroradiology Toronto Notes 2019
• boneandairspace(usethebonewindow):checkcalvarium,visualizemandible,visualizeC-spine (usually C1 and maybe part of C2) for fractures, absent bone, lytic/sclerotic lesions; inspect sinuses and mastoid air cells for opacity that may suggest fluid, pus, blood, tumour, or fracture; status of the orbital floor in cases of facial trauma (coronal series best)
• duraandsubduralspace:crescent-shapedhyperdensityinthesubduralspacesuggestssubdural hematoma; lentiform hyperdensity in the epidural space suggests epidural hematoma; check symmetry of dural thickness, where increased thickness may suggest the presence of blood
• parenchyma:asymmetryoftheparenchymasuggestsmidlineshift;poorcontrastbetweengreyand white matter suggests possible infarction, tumour, edema, infection, or contusion; hyperdensity in the parenchyma suggests enchancing lesions, intracerebral hemorrhage, or calcification; central grey matter nuclei (e.g. globus pallidus, putamen, internal capsule) should be visible, otherwise, suspect infarct, tumour, or infection
• ventricles/sulci/cisterns:examinepositionofventriclesforevidenceofmidlinecompression/shift; hyperdensities in the ventricles suggest ventricular/subdural hemorrhage; enlarged ventricles suggest hydrocephalus; obliteration of sulci may suggest presence of edema causing effacement, possible blood filling in the sulci, or tumour; cistern hyperdensities may suggest blood, pus, or tumour
• pleaserefertoTorontoNoteswebsiteforsupplementarymaterialonhowtoapproachaheadCT
Selected Pathology
• seeNeurosurgery,NS4forintracranialmasslesions
• see Neurosurgery, NS31 for head trauma and Plastic Surgery, PL31 for craniofacial injuries • seeEmergencyMedicine,ER9forspinaltrauma
• seeNeurosurgery,NS24andOrthopedics,OR23fordegenerativespinalabnormalities
Figure 32. Insular Ribbon Sign (Left side)
Hypodensity of insular cortex representing early sign of infarction
Ddx for Ring Enhancing Cerebral Lesion
MAGIC DR
Metastasis
Abscess
Glioblastoma multiforme Infarction (subacute/chronic) Contusion/hematoma Demyelinating disease (e.g. MS) Radiation necrosis
Cerebrovascular Disease (Neurosurgery, NS18)
• pathogenesisofstroke:seeNeurology,N48
• bestimagingmodality:infarctsbestdetectedbyMRI>CT
Table 17. Temporal Findings of Infarction with CT and MRI
Figure 33. CT image of early infarct: hyperdense artery
Time from Stroke Onset
Hyperacute (0-24 h)
Acute (24 h-1 wk)
Subacute (1-3 wk)
Chronic (>3 wk)
CT
Usually normal within 6 h
Edema (loss of grey-white matter differentiation – “insular ribbon sign”, effacement of sulci, mass effect) Hyperattenuating artery “hyperdense MCA sign” repre- senting intravascular thrombus/emboli may be seen in ischemic stroke
Hyperattenuating acute blood surrounded by edema may be seen in hemorrhagic stroke
Increasing edema (seen as hypoattenuation) may result in significant positive mass effect
Resolution of edema leads to increased attenuation of infarcted area that may regain near-normal density and mask stroke “fogging phenomenon”
Encephalomalacia (parenchymal volume loss) appears as hypoattenuation with negative mass effect
MRI
Hyperintensity on DWI within minutes of arterial occlusion due to restriction of water movement indicative of cytotoxic edema Hypointensity on ADC within minutes Hyperintensity on T2/FLAIR approximately 6 h after onset due to edema (loss of grey-white matter differentiation, effacement of sulci, mass effect)
Continued hyperintensity on DWI Hypointensity on ADC reaches nadir at 3-5 d and begins to increase
Continued hyperintensity on T2/FLAIR
Continued hyperintensity on DWI due to “T2 shine through”
Intensity on ADC continues to rise, pseudonormal-izes at 10-15 d, and then surpasses that of surrounding normal tissue Continued hyperintensity on T2/FLAIR
Hyperintensity on DWI/T2/FLAIR progressively decreases
ADC intensity remains elevated
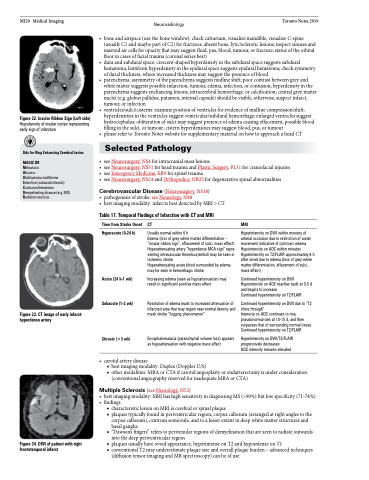
Figure34.DWIofpatientwithright frontotemporal infarct
• carotidarterydisease
■ best imaging modality: Duplex (Doppler U/S)
■ other modalities: MRA or CTA if carotid angioplasty or endarterectomy is under consideration
(conventional angiography reserved for inadequate MRA or CTA)
Multiple Sclerosis (see Neurology, N52)
• bestimagingmodality:MRIhashighsensitivityindiagnosingMS(>90%)butlowspecificity(71-74%) • findings
■ characteristic lesion on MRI is cerebral or spinal plaque
■ plaques typically found in periventricular region, corpus callosum (arranged at right angles to the
corpus callosum), centrum semiovale, and to a lesser extent in deep white matter structures and
basal ganglia
■ “Dawson’s fingers” refers to perivenular regions of demyelination that are seen to radiate outwards
into the deep periventricular region
■ plaquesusuallyhaveovoidappearance,hyperintenseonT2andhypointenseonT1
■ conventional T2 may underestimate plaque size and overall plaque burden – advanced techniques
(diffusion tensor imaging and MR spectroscopy) can be of use
